
Last Thursday, Chris Otts of WDRB News may have been the first to report on Catholic Health Initiatives’ (CHI) most recent quarterly report to its creditors covering the 90 days ending March 31, 2014. Meant to be read in conjunction with last November’s audited annual report, the current unaudited update covers the first full year that CHI has controlled “substantially all of UMCs operations” at University of Louisville Hospital (ULH). The news report focused on the fact that KentuckyOne Health, the manager of CHI’s multiple hospital-related operations in Kentucky, had lost an additional $134 million on its “faith-based” hospital operations over that 90-day period. This stunning loss comes on the heels of an earlier report that KentuckyOne had lost $100 million in the six months ending December 31, 2013.
More than just financial data is provided.
The full report is in the public domain. My reading confirmed what was reported by others. However, I was struck more by other tidbits of information that confirm or add to our knowledge of what is happening behind the surgical drapes hung to to keep the rest of us from assessing the health of this hospital system of which a public asset is part.
[Addendum
Summary of Revenues by CHI Region. (See PDF version for footnotes and definitions.)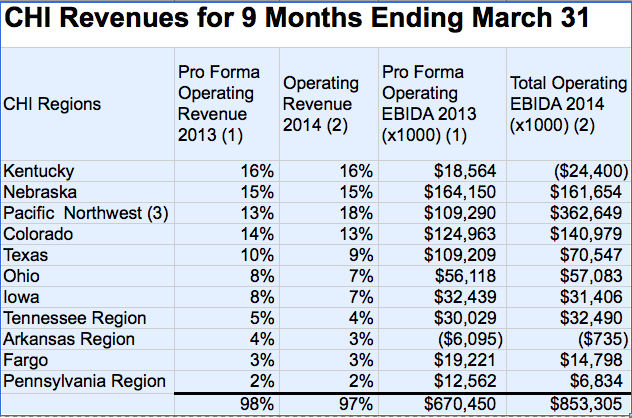
The table above was copied from the report. It compares the nine months ending March 31, 2014 with the same period for 2013. As I understand it, the 2013 numbers do not include revenue from UofL Hospital. Note that “Pro Forma OR” is not the same thing as “Total OR.” EBIDA is shorthand for EBITDA (Earnings Before Interest, Taxes, Depreciation and Amortization) but with the ‘T’ left out because CHI does not have to pay most taxes due to its not-for-profit” legal status. When I looked at Wikipedia for the definition, I was told that “a negative EBITDA indicates that a business has fundamental problems with profitability.”)
Even though the Kentucky Region provided CHI with the highest proportion of its revenue in 2013, its earnings were proportionally very much lower, and in 2014 it yielded by far the greatest loss. It was not a good year in general for CHI– Seven of the 11 regions showed decreased earnings for the reporting period ending March 2014 compared to 2013. Although the Pacific Northwest region looked like it had a great year, the big increase was the result of a one-time affiliation benefit. Without that single item, CHI as a whole would have reported decreased earnings in 2014 so far.
Will something more have to be done?
As the hemorrhaging in Kentucky accelerated, KentuckyOne laid off some 500 employees last March, including quite few from University Hospital– the one hospital in the its Louisville stable that is profitable! Following this action, KentuckyOne’s CEO recently announced, but without supporting details, that the hospital system was halfway towards its goal of fixing its $218 million budget deficit by next July, and that no further layoffs were contemplated in the immediate future. An announcement of further consolidation of unspecified clinical services was made. However, if ongoing losses of this magnitude continue, it may be that the company is be dealing with a moving target of deficit reduction necessity.
Explanations suggested– Details and confirmation needed.
Explanations offered for the losses specific to Kentucky include decreases in patient volumes, problems with physician retention, increases in accounts receivable, and costs related to conversions to new billing systems.
The report also offered a now frequently heard explanation that the payer mix of the system’s Kentucky patients has changed, and that insurers are paying less. This justification is at odds with a recent statement from University Hospital that the Affordable Care Act has led to the desired reduction in its uninsured patients, and a statement in the CHI report itself that charity care provided by the system nationally was down from the same period last year. (See additional discussion about charity care below.)
University Hospital is a money-making machine!
“For the nine months ended March 31, 2014, the operations of [University of Lousiville Hospital] contributed $383.4 million in operating revenues, and $26.5 million of excess of revenues over expenses to the CHI consolidated results of operations, prior to the impact of revenue sharing with KentuckyOne Health.”
How many golden eggs are available?
For years, the University of Louisville bled off millions of dollars annually from University Hospital to support non-clinical activities including research. Claiming that University Hospital was doomed to fail financially unless it merged with Jewish Hospital (and subsequently with KentuckyOne Health), UofL convinced government leadership that to survive it had to merge with its new main squeeze, Jewish Hospital and its CHI ownership. Downplayed was the fact that Jewish Hospital was having its own financial difficulties and had been acquired itself a few years earlier. Now, only one year into the new agreement with UofL, KentuckyOne continues to lose money and is in fact being propped up by University Hospital through a “revenue sharing agreement” The sharing is going in a direction opposite to what UofL expected.
How many and what kind of physicians have actually left?
Listed as an additional reason for the continuing financial losses were a decrease in patient volumes and “physician retention issues.” No specific detail was offered about a loss of physicians. In fact, KentuckyOne’s CEO Ruth Brinkley recently told her employees that efforts to recruit more patients and professionals were showing success. Such gains are apparently not sufficient to cover departures that are becoming obvious to others in the community. I am aware of two high profile interventional cardiologists and a primary care practice that have now signed up with KentuckyOne’s competitors. I do not know how many physicians or other health professionals make up the retention issues. I will suggest one cause of the problem below.
What has University Hospital gained so far from handing its management to KentuckyOne?
The promise of support made to the University of Louisville is mentioned in this report– as it must be: “KentuckyOne Health has agreed to provide capital investments in ULH [University of Louisville Hospital] of approximately $117 million over the first five years of the Kentucky [joint operating agreement.] On June 3, 2013, the Corporation loaned $39 million to ULH, the proceeds of which were used to retire certain outstanding long term debt of UMC”
Presumably the $39 million does not count against the $117 million of investment, but we are reminded that the major reason University Hospital had to take on this the debt in the first place was related to its most recent failed “partnership” agreement. The community is still waiting for an announcement by the University of its first dollar of promised payment from KentuckyOne, let alone how it will be used.
How real is the money promised to UofL?
The additional anticipated financial payment to the University of Louisville proper mentioned in this report (designed to responsibly inform CHI’s financial backers) is characterized using a number of terms that seem imprecise (at least to me) and which confirm my opinion that the amount of money in play was never definitively described to the public. Here is what CHI has to say about the non-hospital pot of money UfoL assumed it would receive. I highlighted in italics the terms that in my opinion should make UofL and the rest of our community nervous.
“ As part of the agreement, KentuckyOne Health has committed to provide various financial support to the University of Louisville over the next 20 years, which as of the acquisition date had a fair value of $217.7 million based upon discounted cash flows and probability-weighted performance assumptions (Level 3 inputs). The value of such contingent consideration will be remeasured to fair value on a quarterly basis, and as of March 31, 2014, had a value of $202.3 million.”
Does it sound to you like UofL is going to get its $217 million? The amount is falling as I write this. I fact, the way I heard it during UofL’s campaign for state approval for its change in management was that a lot more than $217 million was going to come our way. Did I hear wrong? Has UofL not fulfilled its promises to CHI? Is it possible that CHI or KentuckyOne have no money to give at this time? Does anyone other than me think this is an important, even critical matter?
Lawsuits and federal investigations.
After some preliminary language about how all hospitals face complex government regulation “subject to future governmental interpretation,” CHI tells its creditors that “certain CHI entities have been contacted regarding alleged violations of Medicare practices for certain services.” It is not thought by CHI management that the ultimate outcome of these matters will have a material adverse effect on CHI’s consolidated [system-wide] financial position.
The report was prepared before settlement agreements for two federal investigations involving St. Joseph Towson and St. Joseph London hospitals were announced publically. Because these two institutions were mentioned specifically in the report, I am led to believe that other CHI hospitals “have been contacted.” [There was no mention in the report of the St. Joseph London settlement in January 2014, nor of the at St Joseph Towson settlement in April.] I am unaware that other KentuckyOne hospitals have anything to be concerned about.
Charity Care.
When UofL and Jewish Hospital pressed for permission to merge, they promised to provide more indigent care as one of the top justifications. The current report does not break down “charity care” by region or institution. By other report as above, University Hospital is seeing fewer totally uninsured patients. Systemwide, “CHI’s charity care as a percentage of gross patient services revenues decreased to 3.0% for the nine months ended March 31, 2014 compared to 3.4% for the corresponding period of the prior fiscal year.”
Effects of the Affordable Care Act (Obamacare to its disparagers) are probably also playing out systemwide for CHI. However, in my opinion, even last year’s 3.4% seems weak. This is especially true since the definition of charity care used in the report “includes the cost of providing services to persons who cannot afford health care due to inadequate resources and/or who are uninsured or underinsured.” In the past, the terms uninsured or underinsured have been used by some hospitals (in the context of quantifying charity care and community benefit) to include things like contractual discounts offered to insurance companies, differences between cost and payments by Medicaid or Medicare, bad debt in general, or a variety of other “uncompensated” care.
In my understanding, “charity care” is that care provided for which the hospital never had an expectation of payment, no bill is submitted, and no charges are submitted to bill collectors. Charity care does not include all uncompensated care, discounts given to private or public insurance companies, or bad debt. “Underinsured” sounds squishy and its meaning is unclear to me.
Not-for-profit hospitals get tremendous benefits in federal, state, and local law from that status, presumably in exchange for a recognizable and meaningful benefit to the public. I am willing to admit that defining charity care has become a quagmire. In my opinion, 3% is not a fair return, even if a literal definition of charity care were being used. University Hospital was doing better than that all by itself.
CHI and KentuckyOne Health are undeniably religious organizations.
I have heard advocates of the CHI merger and partnership try to deny or minimize the fact that CHI and KentuckyOne Health are religious institutions in order to facilitate acceptance of their take-over of University Hospital management. CHI’s financial report makes it clear that it is a “faith-based” organization” and that “the mission of CHI is to nurture the healing ministry of the Church, supported by education and research. Fidelity to the Gospel urges CHI to emphasize human dignity and social justice as CHI creates healthier communities.” It has become obvious that many medical professionals are uncomfortable subjugating their professional scientific and medical judgement, and that most people are unwilling to hand over control of their personal healthcare decisions to the ministers and dogma of somebody else’s church. The real shame is that our government and civic officials let this happen– indeed were cheerleaders for it– all in the name of “economic development.” We need those officials to act again now to do the right thing.
Many of us do not subscribe to the belief that the gospels of the Catholic Church are the source of all wisdom or ethical belief. Human rights and simple decency alone lead me and others to emphasize “human dignity and social justice” in our practices of medicine and advocacy for public health! I believe that most of the “work-arounds” that allow CHI and the Catholic church and to save face and yet still participate in the lucrative commercial marketplace fail when judged against contemporary medical practice or ethics. For example, I and others have argued that some of the measures used to “work-around” the Church’s prohibition on contraception amount to requiring or inducing patients and physicians to misrepresent facts in the medical record and are therefore unethical medically. In my opinion requiring individual patients and professionals to adhere to its religious doctrine as a prerequisite to providing healthcare in its system is a factor in CHI’s declining revenues in Kentucky and will ultimately cause its hospital acquisition bubble to burst.
Doctors jumping ship?
It would be incorrect for me to suggest that problems with physician retention are due solely or even in major part to conflicts arising between church dogma and science-based medicine. In Louisville, it appears to me that merging Unversity faculty practices with the previously independent practices at Jewish Hospital and giving UofL control of hospital services have not gone as smoothy as the planners desired. I predicted that this would be a problem and by all accounts available to me, things have not gone very well.
Bigger or perhaps even monumental changes in store for University Hospital?
As I prepare this article for posting, other journalists in Louisville are gathering information and sharing speculation about possible earth-shifting changes in the healthcare community of Lousiville. Such things have happened before that affected University of Louisville Hospital. No one more than I wants a stable, accountable, and sustainable future for this community asset in which it can provide high quality healthcare and education. I also venture to say that there is no person or institution that doesn’t wish for us to do better than we are currently. What can the community do to help? Why have earlier University attempts at partnership failed? Are the same mistakes being made over and over? How can we help if knowledge of what is not working is withheld?
As always, If I have made an error of fact, please let me know so I may make a correction. If you disagree with my interpretations, please share your thoughts with the rest of us. Use the email link in the sidebar if you wish to contact me confidentially.
Peter Hasselbacher, MD
President, KHPI
Emeritus Professor of Medicine, UofL
July 1, 2014
[The table of revenues by region and accompanying discussion were added 7-2-2014. The table with definitions and footnotes can be downloaded as a PDF document or Excel file.]
Lay-offs in Arkansas
CHI’s operations in Arkansas were the only other region beside Kentucky to lose money. It is not surprising then to learn that layoffs are in progress in that state. Modern Healthcare reports that recently acquired CHI St. Vincent Hospital in Hot Springs will lay off 91 employees and eliminate 157 positions. That is what happens following mergers and acquisitions such as also occured in Louisville. This is neither good nor bad, but is a predictable way to cut expenses and painful for the employees let go.
Hiring in Louisville?
What I do not understand is how, following painful lay-offs in Louisville earlier this year, an internet job search for openings at CHI in our fair city turns up 503 entries. Is this an artifact of the internet and job advertising market, or, as one employee opined to me, is KentuckyOne is on a “hiring blitz?” Can anyone help me explain this apparent discrepancy?
Something you might want to dig into is how much their IT outsourcing is costing CHI, and their related subsidiaries. There is a saying within CHI that specifically relates to their outsource company: “Certified does not mean qualified”.
Their IT and EHR’s are a mess.
It appears that some of the surgical drapes have fallen and that UofL and KentuckyOne Health are finally beginning to go on the record about the status of their partnership. At the end of this comment is an email from KentuckyOne’s chief medical officer responding to naysayers of whom I must assume I am considered one. I can confirm however, that there are many more than a few of us.
A more comprehensive example that the partnership is feeling community pressure for transparency and accountability is the long article yesterday by Laura Ungar in which all the major leadership players go on the record. I will comment on and attempt to corroborate those disclosures later. For starters, below is an email from KentuckyOne (presumably to professional staff) sent to me by a former colleague who may not be a naysayer, but who is one of many with obviously valid concerns that cannot be brushed off or spun away.