
How will we know if we are still ahead?
It had to start sometime, but pressure from partisan and a variety of other assemblies have surely advanced the nation-wide schedule for lifting restrictions of non-medicinal management of the Covid-19 epidemic. It is happening in Kentucky too. While there are state differences in degree, the number of new cases identified continues to increase overall. We are “bending the curve.” Because availability of viral testing continues to be limited, as more testing done more cases will be found. How best should we monitor our populations to detect, localize, and quantitate any significant second peak in the curve of disease incidence? I cannot say that I know!
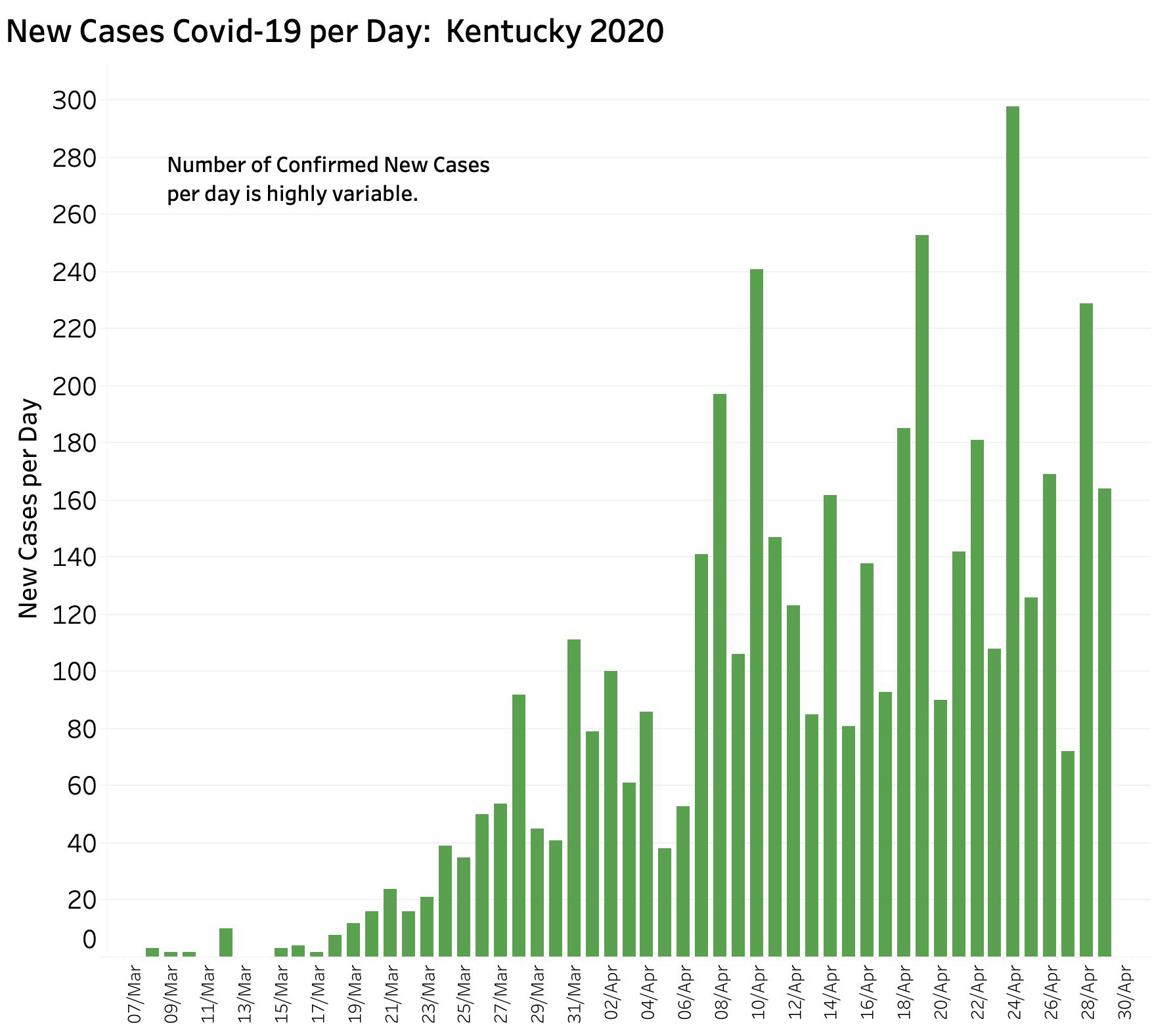
Kentucky has been fortunate to have acted early and aggressively to deal with our rising number of cases. Despite relative success compared to other states, the number of known cases in Kentucky is rising and will continue to do so while our still-modest ability to test for the virus increases. A 7-Day rolling average of daily new cases remains high. Timely identification of new cases will be essential to deal with the brushfire outbreaks that are certain to occur in the months ahead– whatever we do. Depending on the day of the week, the number of tests done, and reporting from new hot-spots, the number of new cases per day varies widely, making predictions uncertain..
What other measures could we track? Some potential independent statistics that are less directly correlated with frequency of testing, and which we are already collecting include deaths and hospital utilization. These are, however, manifestations of more severe disease and will necessarily lag in time from any overall increase in viral infections.
About deaths.
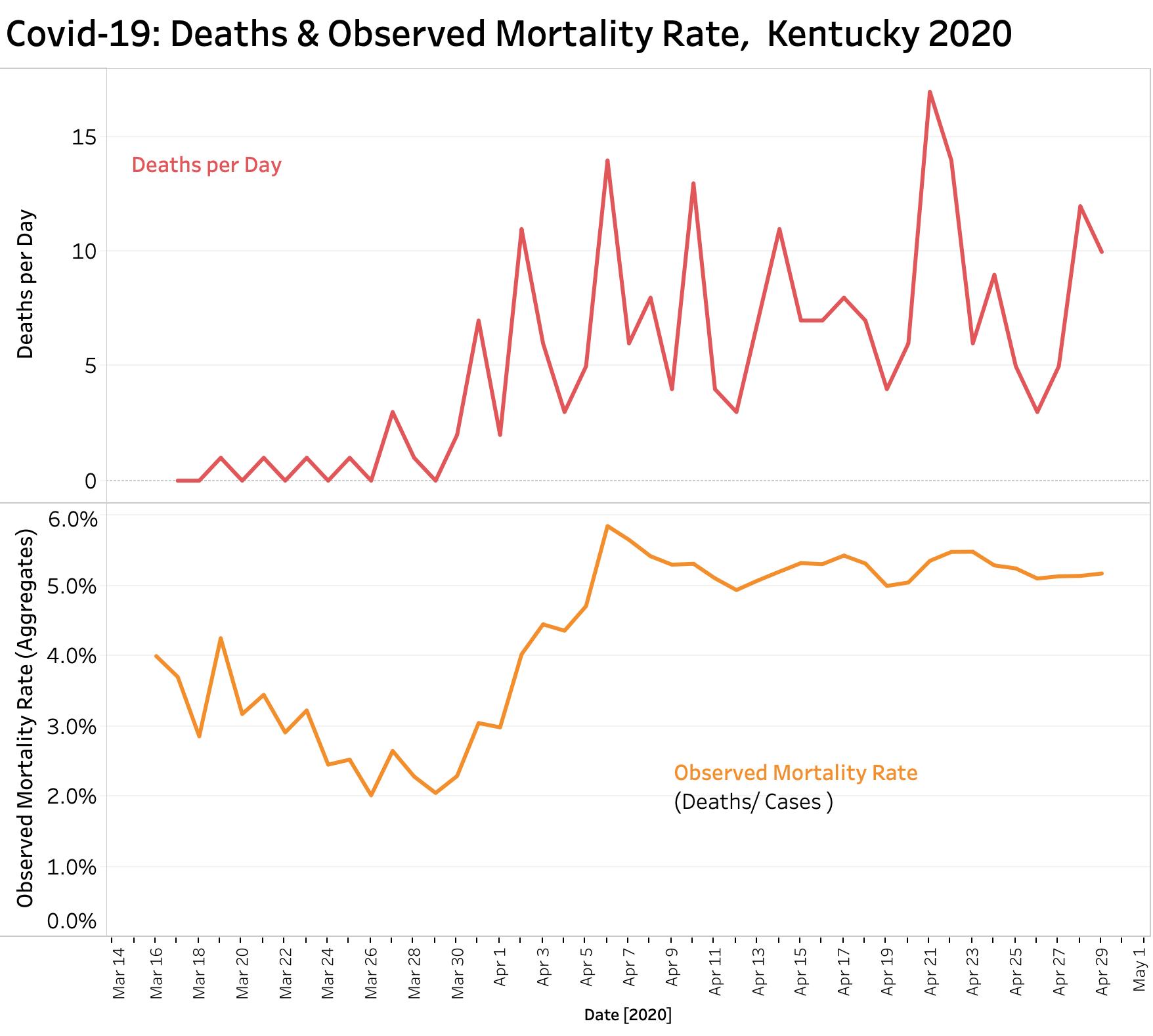
Deaths attributed to Covid-19 are perhaps the most objective indicator of the presence of disease but will lag the onset of an actual new outbreak and will depend very much on timely reporting of accurate diagnoses from a well-integrated network. I am not confident that we are there yet. The number of reported deaths has varied considerably from day to day also requiring some form of averaging to identify a trend. (See figure below demonstrating the volatility of the number of reported daily deaths in Kentucky.)
Not all deaths from Covid-19 will be recognized as such. It has been shown that when compared to previous years, current overall death rates can be much higher than accounted for by Covid-19. The excess deaths contain both unrecognized Covid-19 infections, and deaths caused by the usual disease actors like heart disease or stroke in individuals who were afraid to seek medical attention, were squeezed out, or were excluded from access to medical care in the first place.
Hospital and ICU utilization.
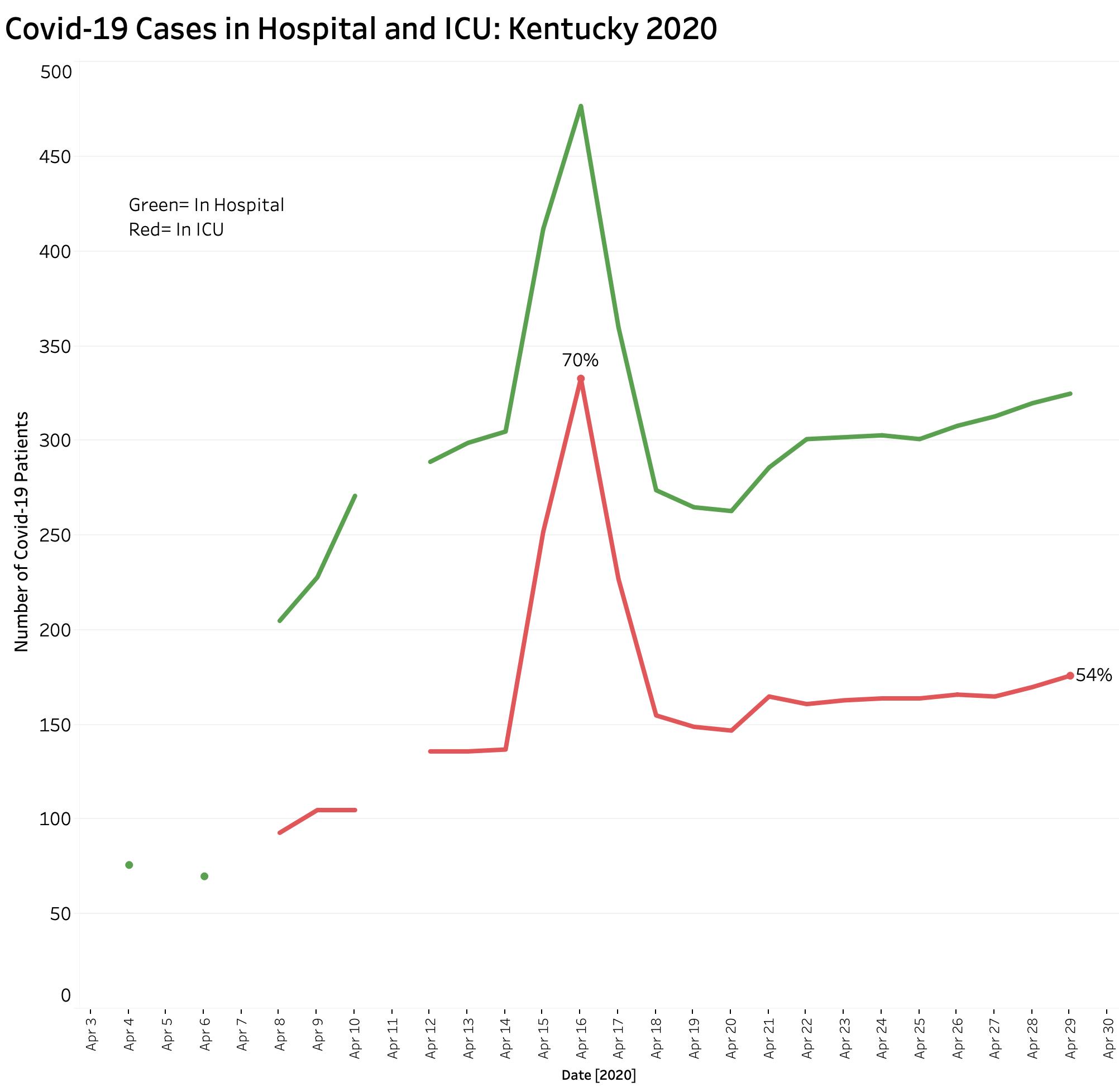
Even as tip-of-the iceberg that it is, careful monitoring of hospital utilization is important to watch, both as an indicator of disease prevalence in the community and to warn of capacity overload. Hospital numbers alone will not detect the asymptomatic super-spreader. Based on hospital-utilization numbers released during the Governor’s daily briefings, hospitalizations and ICU utilization related to Covid-19 rose rapidly from early April to a peak on April 16, then settling down to a slowly rising number. The number of patients in ICUs tracks closely the total number of hospitalized cases at any one time. At its peak on April 16, 70% of hospitalized Covid-19 patients were in ICUs. Since then, that proportion has decreased, hovering around 54%. Note however, that the distribution of hospital beds, and in particular ICU beds, varies greatly throughout the state. Following hospitalizations may be less useful in less populated areas and will in any event not be an early indicator of a recurrent outbreak.
How many cases are already out there?
We do not even know what the current baseline is of Covid-19 incidence is. Up to now we have been testing only the sickest individuals, those taking care of them, or those otherwise at high risk. The percent of aggregate viral tests that are eventually reported as positive has hovered between 8 and 9% for the last two weeks. Because of lags in reporting both the number of daily tests and the numbers of cases, the percent positive jumps around dramatically on a daily basis. Such variation in numbers also requires looking at some form of averaging to begin to smooth out curves and allow predictions.
Final comments.
Covid-19 is an exceptionally infectious agent. Wherever two or three are gathered together, the disease spreads efficiently; be this is in a nursing home, a ship, a place of worship, or a bridge club. Based on Kentucky’s numbers, 5.2% of cases identified so far by viral testing have already died– a number that has not been decreasing despite efforts to increase testing. The stakes are high.
I am not aware of all the statistics the Commonwealth may be collecting. I have access only to what has been made available in the evening public briefings. I have confidence in our Governor and his public health team. I have reservations that the things we have been measuring are sufficiently sensitive or timely for what is needed. Moreover, I am concerned that in our Commonwealth of 120 diverse counties; that our multi-compartmental system of public health agencies and our non-system of siloed healthcare providers may not be integrated enough to provide sufficiently timely notice of a resurgent outbreak. What we must have is a coordinated, statewide, and boots-on-the ground public health presence that can identify and react to emerging geographic hot-spots of disease. This public health presence must have both the ability and authority to trace previous and subsequent contacts of identified infections and to effectively enforce appropriate quarantines. In my opinion, we have a demonstrable way to go in these regards with respect to manpower, funding, and authority. Kentucky plans to loosen its epidemic control restrictions gradually. That is certainly appropriate. We will also learn by watching what happens in those states currently opening up their doors more widely.
I will continue to update the Tableau Public data visualizations, but will likely tinker with or add views.
Peter Hasselbacher, MD
President, KHPI
30 April 2020