
Presence of holiday weekend with big-time concerts and decreasing reporting protocols make forecasting iffy.
On May 31, the staff of the Kentucky Department of Public Health gave an online update to practitioners. Since there are no longer any weekly, let alone daily updates from the Governor’s Office, this well-done authoritative session, combined with the published weekly online updates from the KYDPH are now my best sources of information about Kentucky’s Covid-19 epidemic. Following are some of the highpoints
from Tuesday’s presentations.
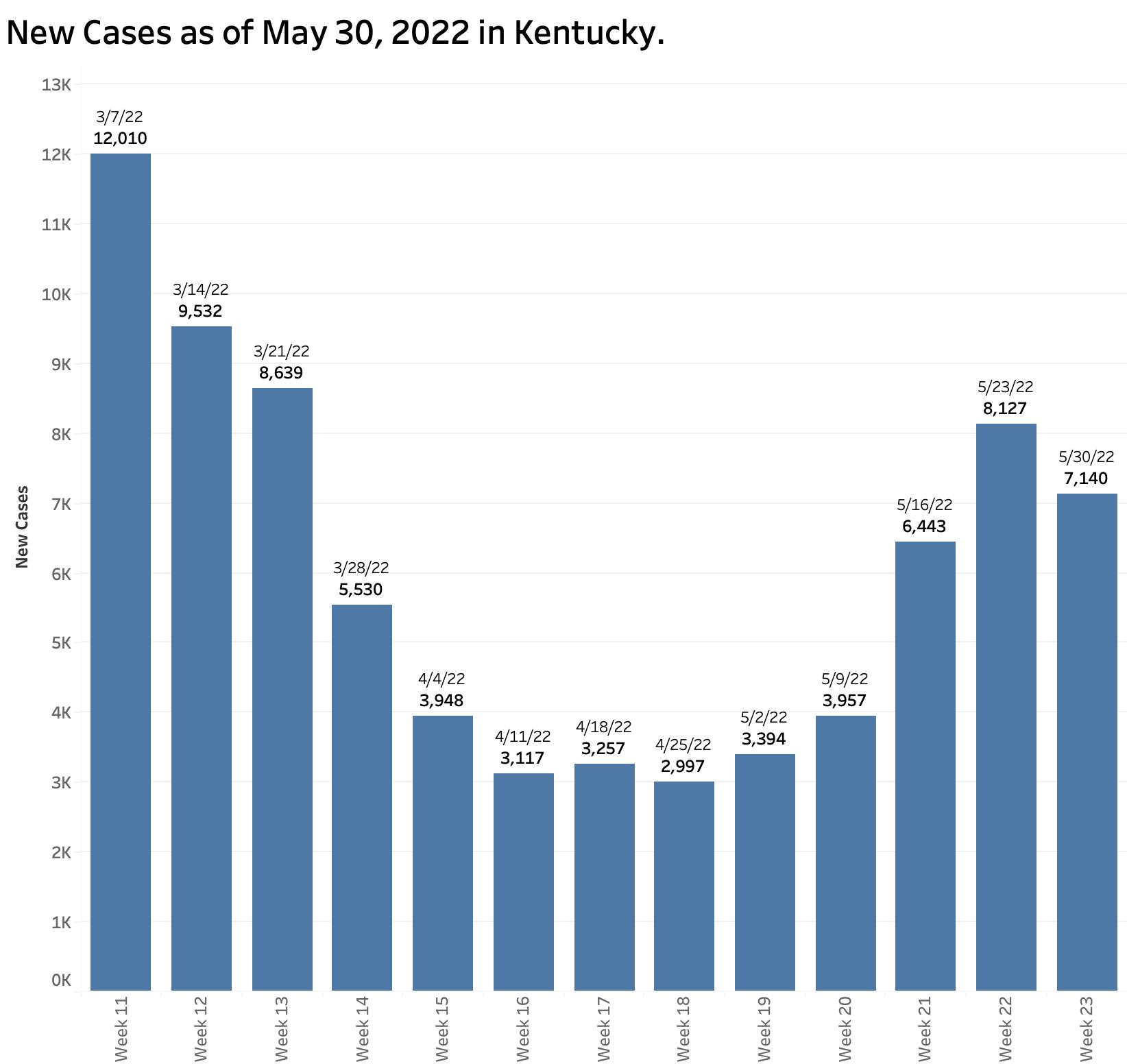
Cases: The 7-Day total of new cases ending May 30 was 7140, the first decrease since the incremental current surge began 5 weeks before. I am not sure what to make of this as previous long holiday weekends were often followed by a period of lower testing and reporting. The number of PCR tests performed last week was essentially the same as the week before. The bulk of new cases reported has increasingly come from this subset of PCR tests reported electronically to the state. For the past 5 weeks, more than 60% of new cases presented to us and to the CDC came from PCR tests. Last week, the figure was 78%. This increasing representation from reported positive PCR tests is compatible with the large and increasing number of antigen office or self-tests that are not reported one way or the other to anyone.
I assume that at least some of the reported PCR tests originate from hospitals. In recent weeks, Kentucky hospitals are no longer required to report “suspected” cases of Covid-19, presumably to cull out individuals who come to a hospital for non-Covid reasons and are found to be positive. The actual number of new cases is surely several multiples of what is reported above. While it would be nice to be sure that a Derby wave of cases is passing, it remains to be seen what happens following the Memorial Day holiday with its large-scale music festivals and other public activities.
Deaths: The 37 deaths reported are by far the lowest in a long time. Previous exposure to Corona virus antigens through infection or vaccination is protecting people from the worst outcomes when infected by the nearly ubiquitous OmicronJunior strain (BA.2) which is more infectious but perhaps less deadly –to the young and vaccinated anyway.
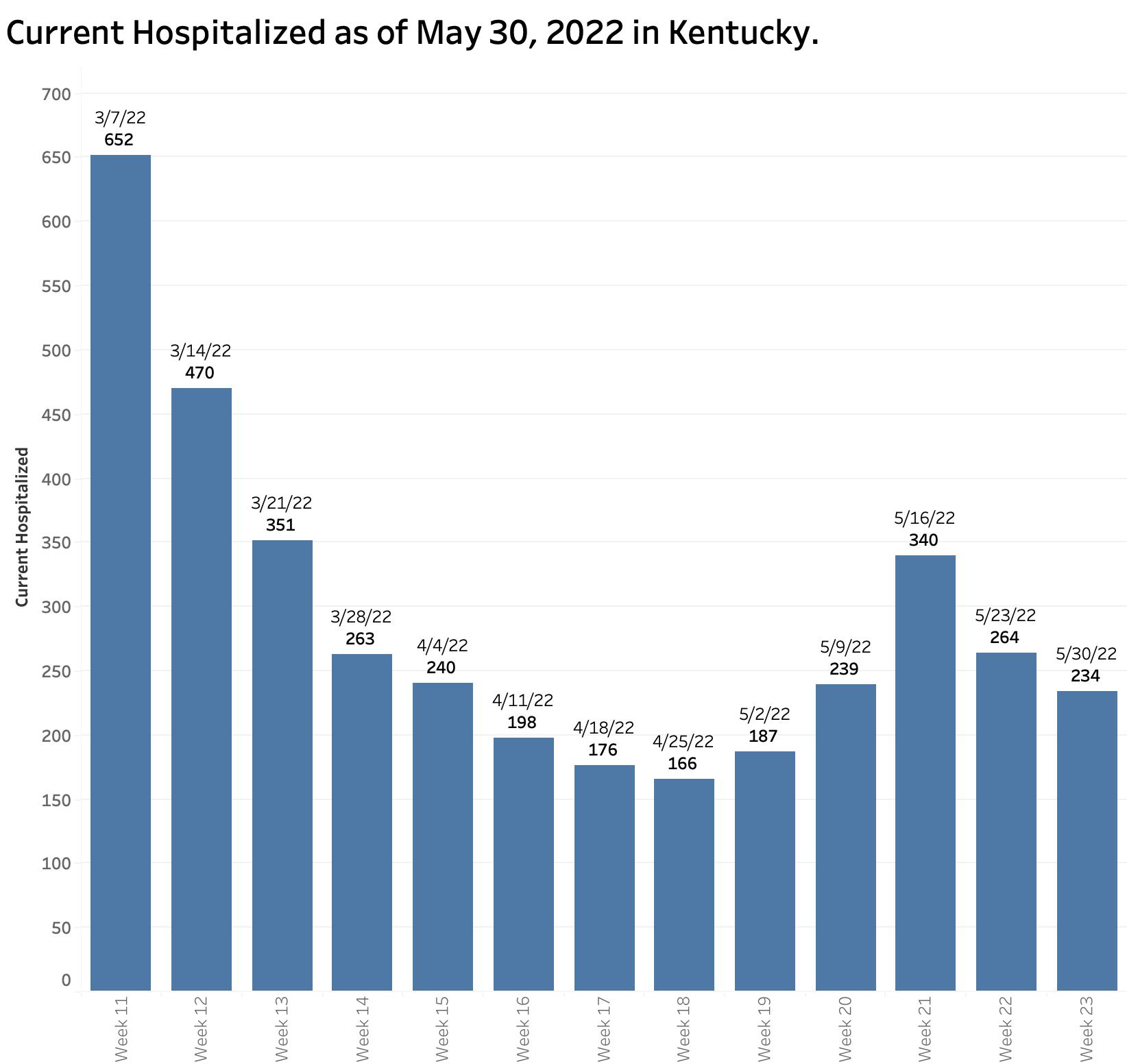
Hospital Utilization: Current hospitalizations jumped up significantly after Derby but have been falling for the past two weeks. We are told that some of this is due to suspected cases not being included in the counts. Both current ICU and ventilator numbers have been bobbing up and down at low levels for the last 6 or 7 weeks. That is good! I would like to think that these tallies are among the most reliable available to us. These would be low for the same reasons that deaths are. We are told that hospital reporting of Covid-19 is getting better across the board with a new system. These good numbers are not evenly distributed throughout the state for reasons discussed in earlier articles. Some hospitals are feeling Covid pressure in their bed- and ICU availability.
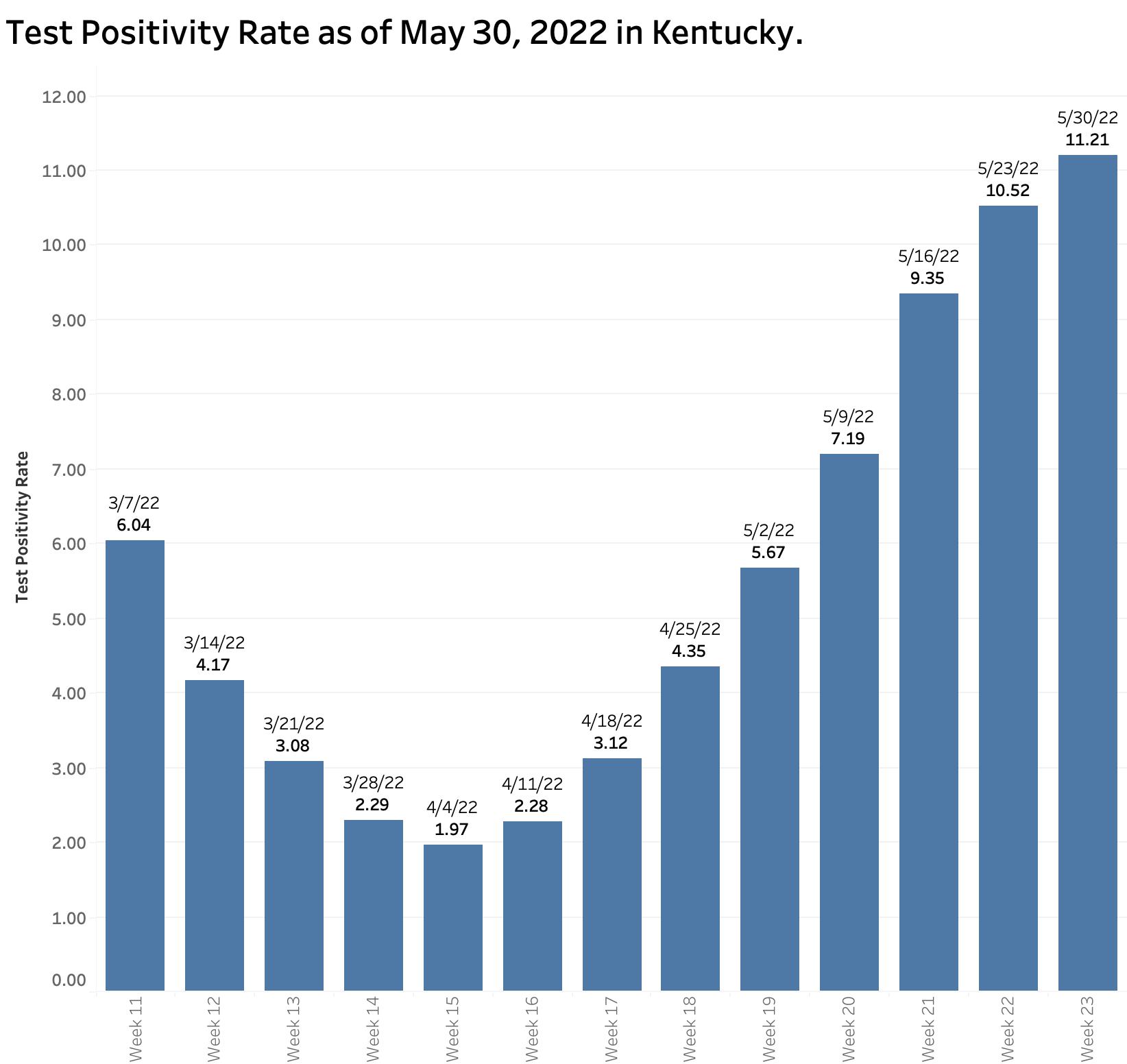
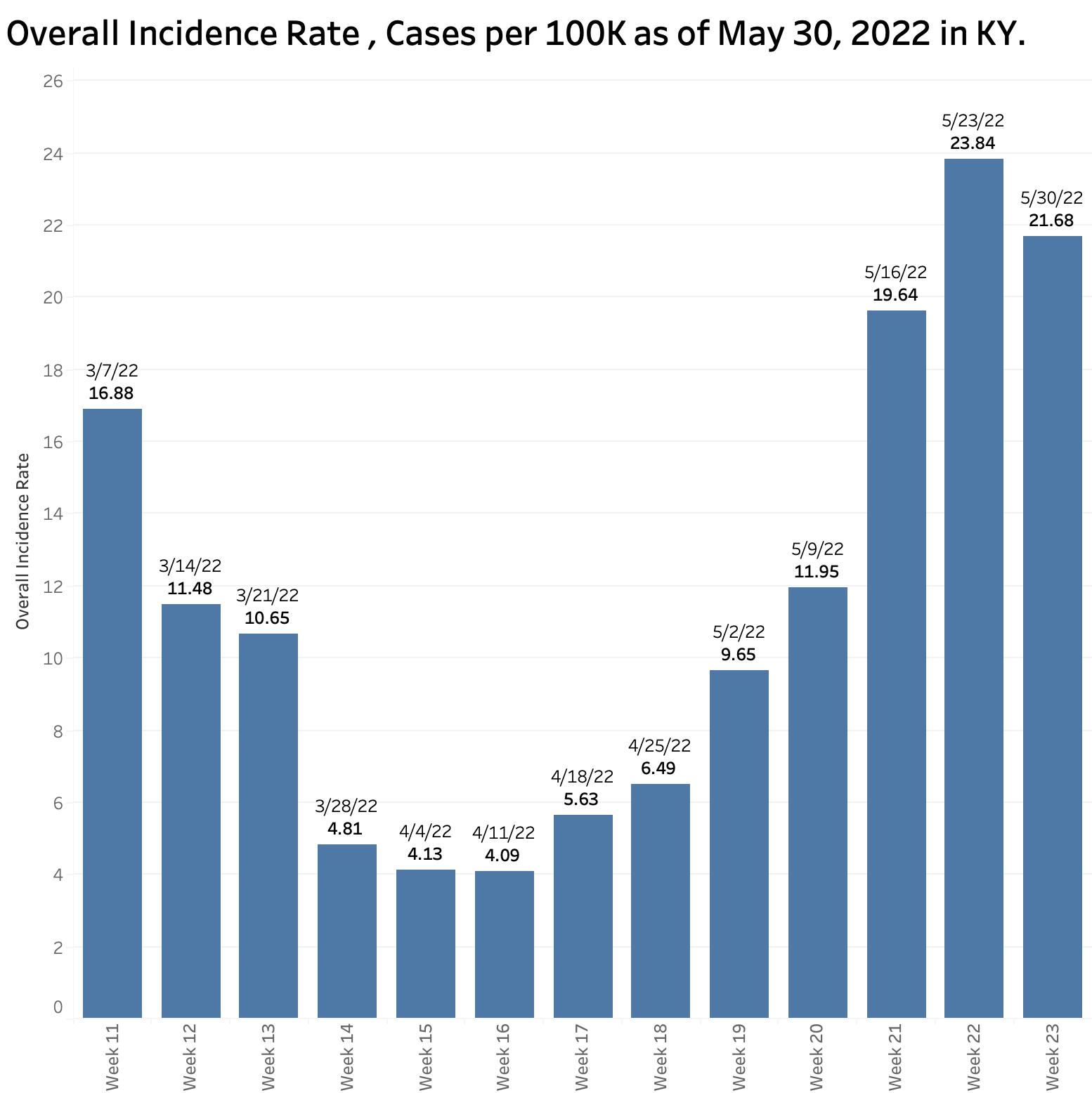
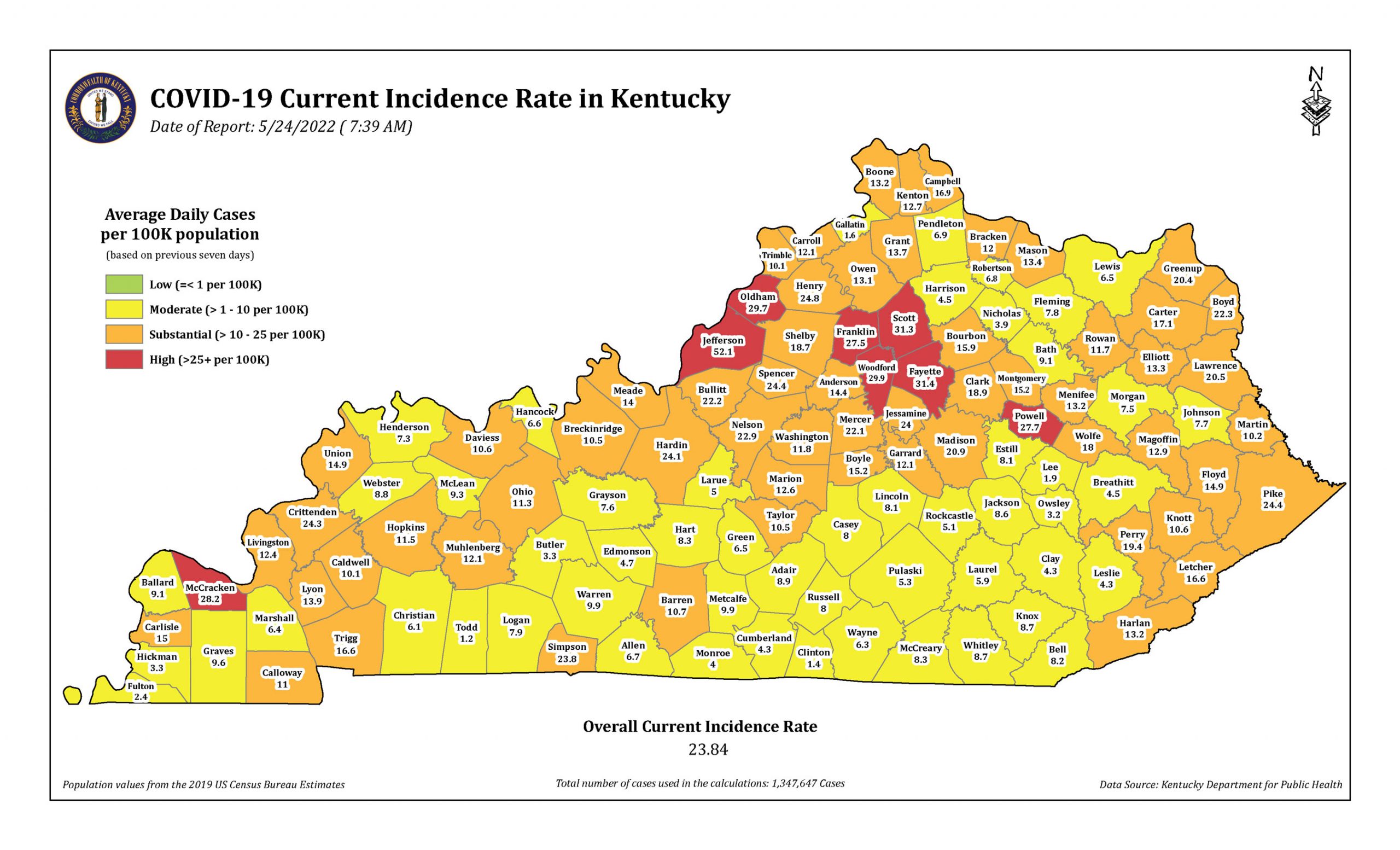
The case and other counts above comprise the total for all 120 counties for a week. However, more than half of our counties had substantial or worse incidence rates over the last 7K days. Eight of those are at a “high” level with more than 25 cases per 100K. The current incidence rate for the state as a whole is 23.8 cases per 100K- almost high. (I am not sure at this moment whether the time denominator here is per day or per week.) In any event, the state-wide incidence rates of new cases these last three weeks were the highest since early March when weekly reporting became the state’s standard. The Test Positivity Rate is still climbing relentlessly, now at 11.21%. We are still churning out new cases!
Vaccinations: Kentucky as a whole is not one of the most vaccinated states. We have done best in our “older” at-risk population older than 50 or 65 years for both the regular series and boosters. The KYDPH presentation offered good evidence that having a primary series completed gave protection against becoming a recognized case and remarkable protection against becoming a death statistic! Those receiving at least one booster were at 15.7 times lower risk of dying. More than 60% of cases of deaths were in the unvaccinated population. We are told that 90% of deaths of individuals under 60 years old were unvaccinated. That is a lot. Receiving a booster gave even more protection. It remains the case that most deaths occur in those older than 60. To prove the protective point, 68% of those older deaths were in the unvaccinated elderly.
Upwards of 50% of employees of nursing homes are still unvaccinated. Explain to me again why vaccination of hospital workers, nursing home staff, or prison guards for that matter should not be subject to mandatory vaccinating? This virus is killing our grandparents! It wasn’t family visitors that brought most of the virus into the old folk’s homes.
Booster shots for all eligible individuals are recommended. Extensive tables and decision tree charts are offered for providers. The different relevant variables of time, age, specific vaccine and the like are almost impossible to keep in my head. I personally got a second booster before an international trip earlier this month. It give it credit for keeping me alive and out of the hospital!)
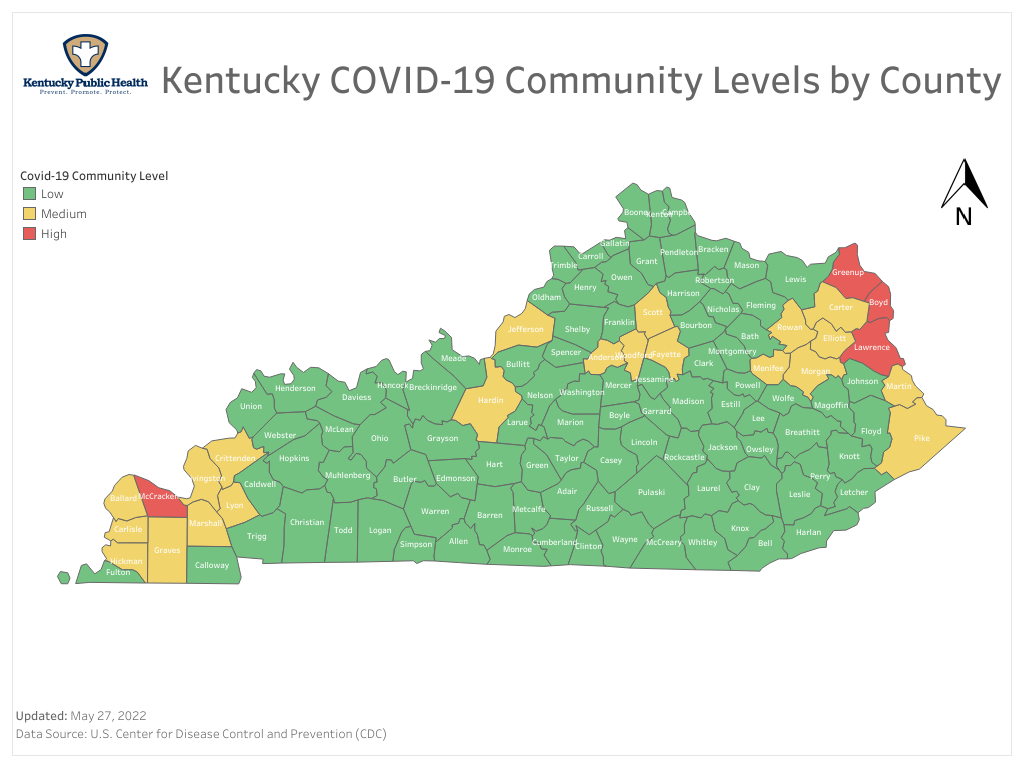
CDC Community Level Indicator Maps: I still don’t know how to use these mostly green-colored county maps. While there are 4 counties in the most recent Community Level Map that are in the red, only one of these is also red in the Current Incidence map summarized above. (Surprising to me, for the first time, I heard the Community Level Map described as a preview of what it yet to come.)
Multisystem Inflammatory Syndrome in Children : One of the worst outcomes of Covid-Infection in children and some adolescents is the poorly understood MIS-C. Kentucky has had some 114 cases of MIS-C since the onset of the epidemic. Most are unvaccinated. Fortunately this complication is rare. Fewer than 1% of MIS-C patients die. However, they can get really sick, including need for ICU and ventilators (63% and 10% respectively). There remains much to learn. Non-white kids get more than their share of MIS-C. In my mind this is just another reason why everyone (of any age) deserves access to the same high-quality healthcare system. This is decidedly not the case presently where there are too many undertreated and overtreated people alike!
Therapeutics- Paxlovid Rebound: There was much presented about treatment of early Covid-19 infection including Paxlovid. “Rebound” of symptoms and recurrent test positivity can occur shortly after the 5-day course of the drug ends. Fortunately, people seem to do fairly well in the end. “Rebound” may be more common than predicted for this and similar treatments and needs to be monitored more closely including whether or not the rebounder is still infectious!
Other Infectious Diseases: Updates were offered for Pediatric Acute Hepatitis of Unknown Etiology. Kentucky has reported 3 or 4 cases so far. Practical advice was given to providers about when and how to report suspected cases. This illness remains globally as a big and serious mystery. We can be reassured that our public health team is on the case. Legislators– give them the financial and other support they need to protect our children Don’t mess it up.
Monkeypox: A good review of the global and national situation was given. There are cases in the USA but none yet recognized in Kentucky. There is no reason to believe it will not show up. This is an infectious disease related to smallpox. It has evolved new mutations at an unexpected rate. What damage is does and what we can do about it remain to be seen. Consideration is being given whether there is a role for smallpox vaccination. Just one more emerging virus making its way around the world when we need it least, or a predictor of what is yet to come in our unsettled planet? Explain to me why we do not need a strong public health system integrated into the healthcare system we all use?
Influenza is making the rounds with an atypical cycle beginning mid-March instead of the usual January or February. Now that we are increasingly letting our respiratory-illness guards down it remains to be seen what will happen. Last year’s vaccine was not a good match for the strain that emerged. Good thing we were taking care of respiratory business in general and that total case numbers were very low. Still, immunization for influenza this fall is recommended. I will get my shot. Covid and Influenza will still be with us along with their fellow lung-loving travelers. As the Game of Thrones books and TV series warn, “Winter is Coming.” Winter brings respiratory diseases which when I was an intern in 1972 and long before were named as “Captain of the Men of Death.” They still are, even in the best of times.
Peter Hasselbacher, MD
Emeritus Professor of Medicine, UofL
Kentucky Health Policy Institute
3 June 2022