
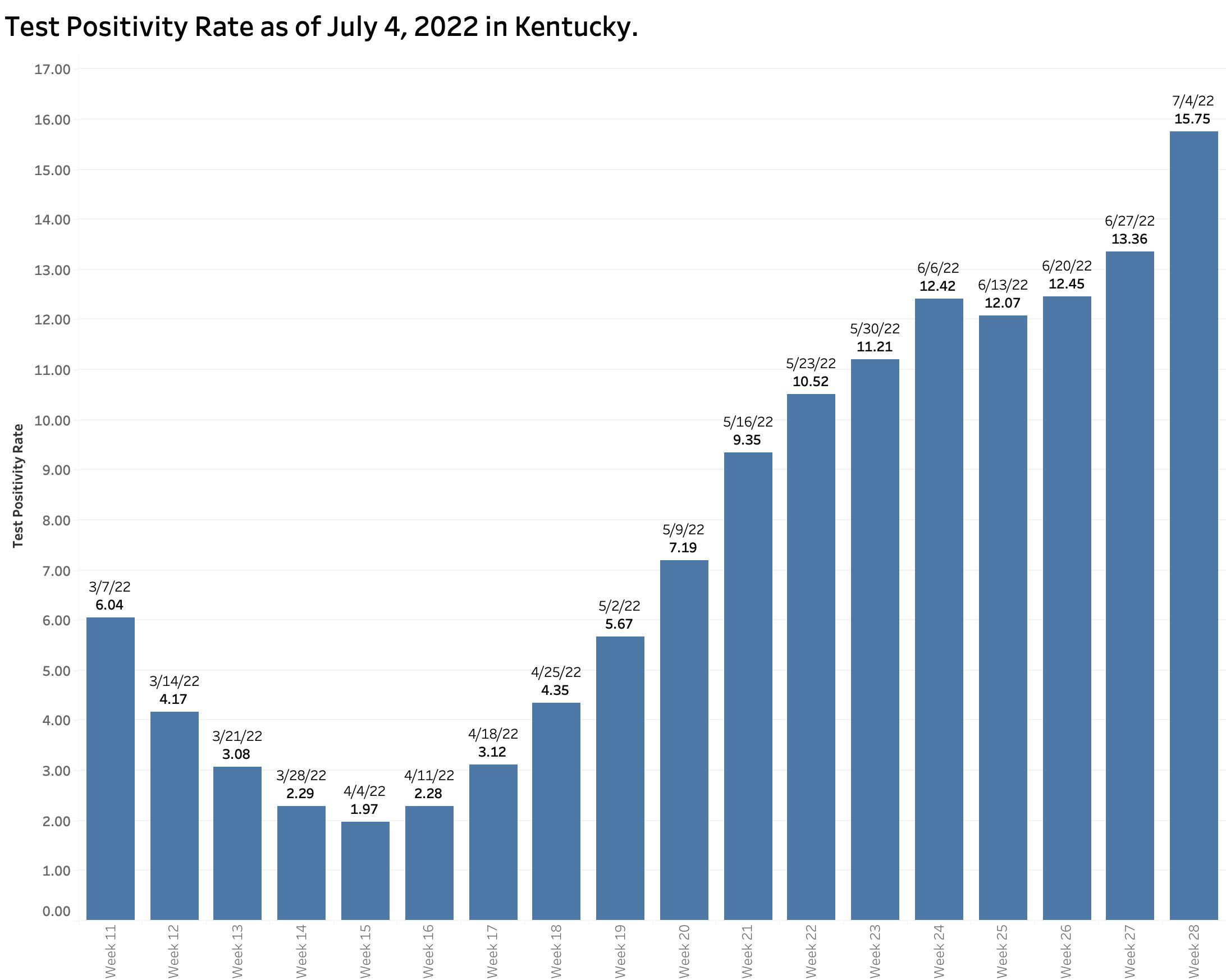
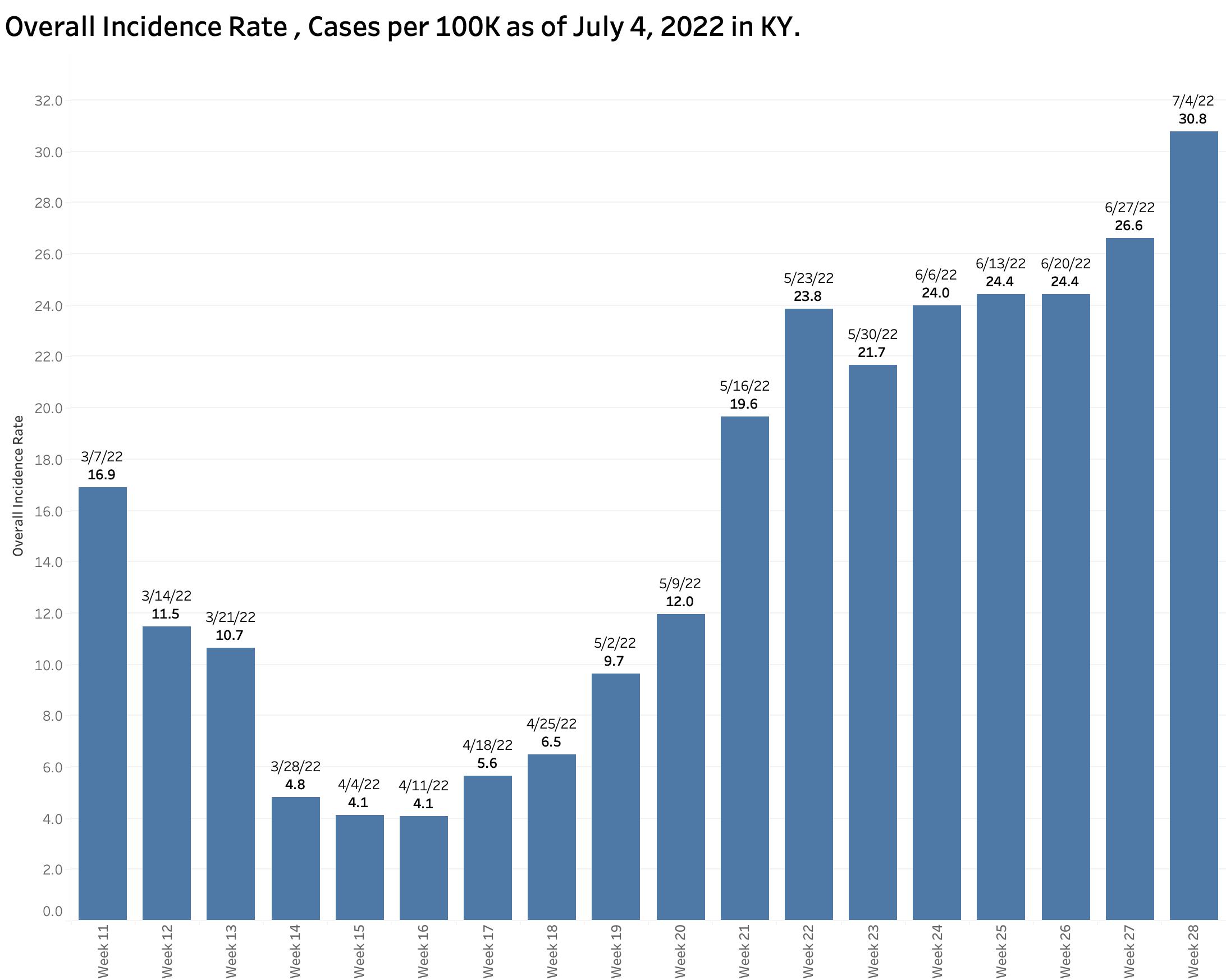
The intervening Fourth of July Holiday and another bump in the road about how cases were counted made the number of new cases reported less indictive of the actual state of Kentucky’s epidemic expansion. The July 4th report of Test Positivity of 15.75% is the highest since mid-February with a string of uninterrupted increases since April 11. Similarly, the Overall Statewide Incidence Rate is also at a new peak of 30.8 new cases per 100K population. Both these previously reliable indicators continue to rise at an exponential rate.
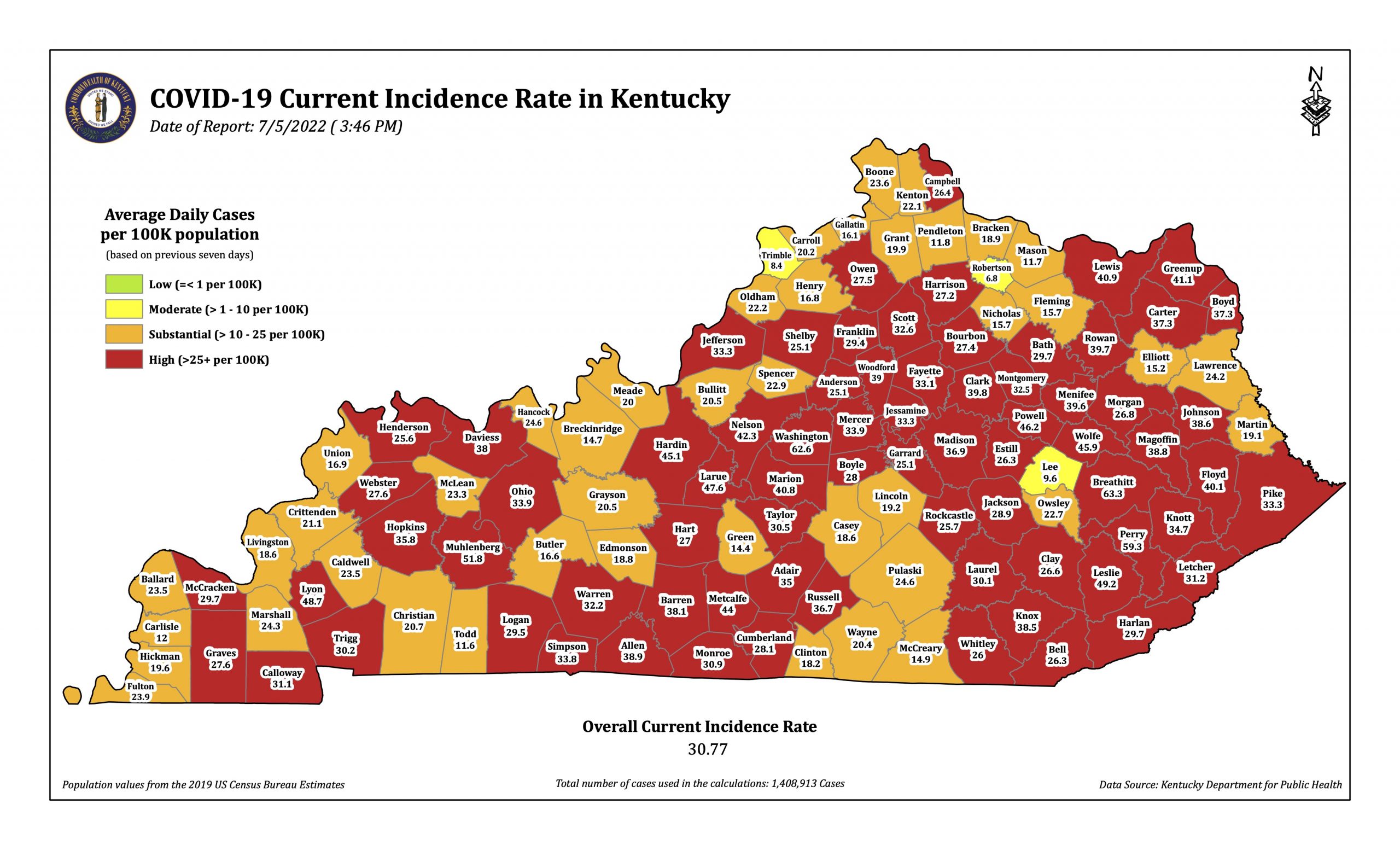
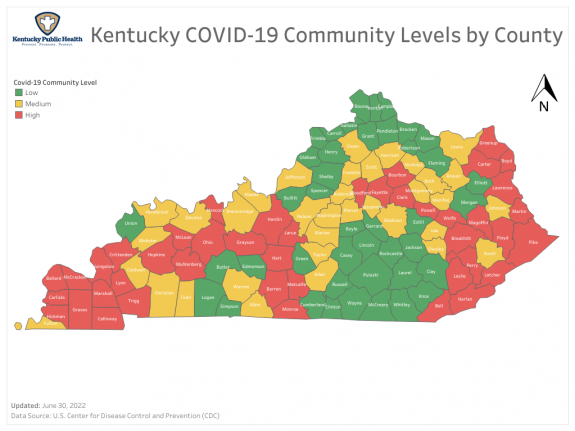
The state as a whole and 74 of its counties are in the red “high” category with another 43 in “substantial” for a combined 97.5% in these highest two categories. Only 3 counties are currently in the moderate category, and none are in the green! Even the CDC Community Level map of June 30 which emphasizes hospital utilization is turning the corner with more “red” counties.
New weekly cases continue to rise, but beginning with the report weeks of June 20th and 27th there was a change in the way cases were reported. An apparent backlog of cases whose onset of infection was more than 30 days earlier were no longer reported as “new cases” but were instead added to the total so they did not missed entirely. For the two weeks mentioned above, 3159 cases of Covid-19 were thus excluded from “new cases.” I do not know how far back this distorting issue is significant, but we have seen similar delays in reporting before. It speaks to the nonuniform method of collecting data from the many different public health departments in the state. Obviously, such changes degrade the timeliness and reliability of reported data necessary to estimate epidemic activity.
Other reasons for lower case counts.
Over the last three weekly reports, the number of PCR viral tests has been decreasing. Since currently 74% of our new cases are identified by PCR testing, fewer tests mean fewer new cases discovered. It is generally assumed that new cases are increasingly undercounted due to abundant use of antigen tests at home and elsewhere. Epidemic “fatigue” is also playing a role. Now that school is out, the proportion of cases in individuals 18 and under is dropping, currently at about 12%. At a peak of 26% of all new cases in March, it is clear that school-age people are major players in our epidemic activity.
It is likely that one of the new Omicron variants BA.4 or BA.5 is pushing things along. Experience in other places suggests that hospitalizations and deaths will not rise as rapidly. That appears to be the case for us as well. In part this reflects the protective effects of prior infection or immunization. It remains true that the unvaccinated person or Covid virgin is at greater risk in general. However, even milder cases are disruptive to the fabrics of our social and economic community.
I have little more to add. Hopefully things will sort themselves out. A sceptic might suggest that since the state’s public health leadership and Governor’s office are essentially prohibited to take any meaningful action in the face of worsening epidemic expansion, why bother to count anything? I would not go so far. Even if individuals and local communities are being handed primary responsibility for managing their public health matters locally, they need geographically relevant meaningful information in a timely manner. I believe that enough sensible Kentuckians will change their behaviors in response to reliable information to make a difference. To that end, we need to understand and trust the information provided.
Peter Hasselbacher, MD
Emeritus Professor of Medicine, UofL
Kentucky Health Policy Institute
6 July 2022