
Focus on Louisville.
Although in a previous life as a clinician I always cared for a few children by default, I cannot claim to have insider or expert knowledge about the operations or politics of children’s hospitals. Nonetheless, when I was a hospital lobbyist, I always made a point of bringing visiting legislators through Norton Kosair Children’s Hospital to brag about the fruitful cooperation between the University and a private hospital in which no patient was ever turned away for inability to pay no matter how long they stayed. (I would have to think twice before doing that today.) I therefore take the opportunity provided by the current University of Louisville/Norton Healthcare dispute to familiarize myself with pediatric care in the state.
Going to the numbers.
It should be no surprise to my readers that as an old scientist, I like to look at the numbers. I can’t spell or remember names, but patterns emerge when I look at tables of data causing me to want to know more. So it was when I looked at the distribution of Neonatal Intensive Care Units throughout the state. The obvious next step was to take a closer look at how those beds were being filled with patients. I have already posted relevant pages from hospital utilization data collected by the Cabinet for Health and Family Services for 2012. Lets take a closer look. For simplification, and to get an initial handle on what the data might tell us and what it cannot, I extract here the numbers for births and special care bed admissions for children in Louisville, and for comparison, the University of Kentucky. (Download Table as PDF.)
Not all data equally useful.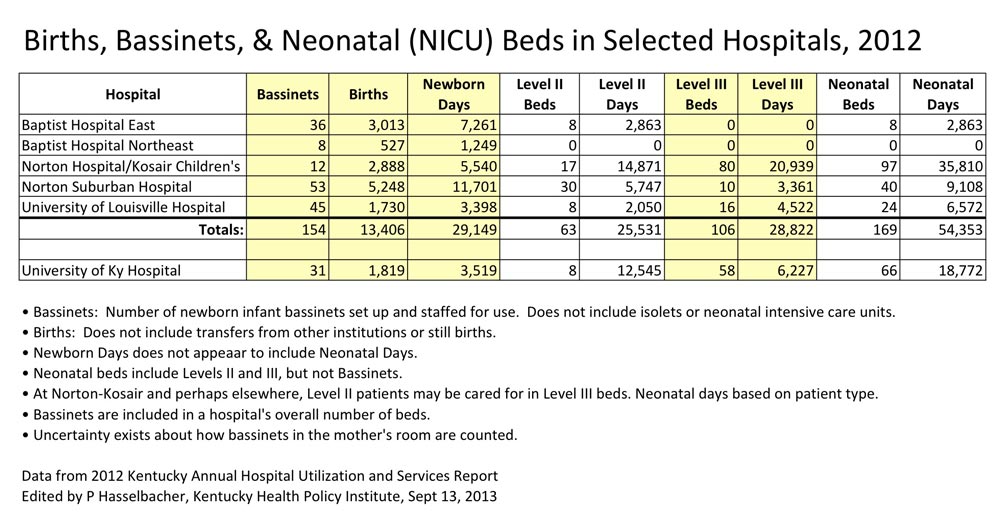
It is immediately apparent that there are problems with the numbers. For example, I do not even bother to present the bed occupancy rate for NICU beds because the footnotes to the report make it apparent that different hospitals use different criteria to identify what children are cared for where. How for example can the University of Kentucky have a 424% occupancy rate for its Neonatal Level II beds– four babies to the crib? This is not a trivial matter, because utilization rates in hospitals are one of the important factors used by the Certificate of Need process to decide whether requested additional services by hospitals should be granted.
Collecting good data is difficult.
When I was a laboratory scientist doing the statistical analysis of the results of a study, we often used the illustrative phrase, “Garbage in, garbage out” to reinforce how important was the process of designing a study, defining its terms, collecting the data in a careful uniform manner, and making sure not to over-interpret the results. The same principle applies for quality, utilization, and policy research. I do not imply that the data in the state’s report is garbage, but it is not a scientific study and is only as useful as the numbers sent by Kentucky’s providers. I therefore approach this table as an “experiment of nature”– a spontaneous event from which I hope to learn something, if only the next questions to ask. Here is what I see.
Number of Births.
In the KIPDA Development Area in which Jefferson County dominates, Norton Hospital downtown and Norton Suburban are the preferred places to deliver babies. The two hospital complexes between them host 61% of births and 59% of newborn days. Baptist East in Louisville’s suburbs is the second-most busy hospital with 22% of births and 25% of days. Despite having almost as many bassinets as Norton Suburban, the University of Louisville Hospital has only 13% of births and 12% of days. Despite honest and expensive efforts to make it a more attractive place, University Hospital is not currently a preferred place for women to deliver. This phenomenon is in largest measure a consequence of what we have created in this community by segregating most of the care for the disadvantaged to that institution. We all share in what I consider to be the blame for permitting this to happen, indeed to institutionalizing it.
Number of Special Care Beds and Days.
We have already noted that Norton Kosair has the lion’s share of high-level Neonatal Special Care beds in the state, let alone in Louisville. (In the 2012 state utilization report, Level III and Level IV NICU beds are combined into Level III.) In the KIPDA area, Norton Kosair has 57% of the special care neonatal beds, but 66% of neonatal bed days. Norton Suburban has 24% of special beds, and 17% of days. Baptist has 5% of beds and 5% of days. University Hospital has 14% of beds and 12% of days. It seems obvious that when these numbers are compared to the number of births, and from the discrepancies between the numbers of special care beds and bed days, that sick babies are being transferred to Norton Kosair from other hospitals. That is how it should be.
University of Kentucky.
Norton Kosair and its adjacent downtown Norton Hospital are busier than the children’s service at the University of Kentucky in all these measures. UK has more standard-care bassinets, but fewer deliveries and fewer newborn days. Similarly UK has fewer special care beds and neonatal days than Norton Kosair. Nonetheless, inspection of the numbers from the Bluegrass Development Area reveal that while UK hospital has plenty of competition for delivering healthy babies, the large bulk of the sickest babies from that area and from elsewhere are being sent to UK. UK is filling the same need for its part of the state as Norton Kosair is for us. While UK might not want to admit it, Norton Kosair provides it necessary back-up support for some of its most difficult pediatric cases. Why would we not want these two organizations to work more closely together?
I will now take my own advice not to over-interpret the data and stop. It is clear to me that Norton Kosair Children’s hospital is the lynchpin of Kentucky’s pediatric health care network. I invite anyone who is willing to justify bringing it down to tell us why in the comments section below. You need not give an email address, but I will not accept a comment for which you do not identify yourself. Stand up for what you believe. If you are troubled by the direction the University of Louisville is going as I am, tell us that too.
Respectfully,
Peter Hasselbacher, MD
President, KHPI
Emeritus Professor of Medicine, UofL
September 13, 2013
[Addendum: I plan to add some graphs to illustrate the relationships discussed above.]