
I do not believe we are in any position in Kentucky to let go of the alligator we are wrestling. I am still waiting for better clarity of what we are actually facing.
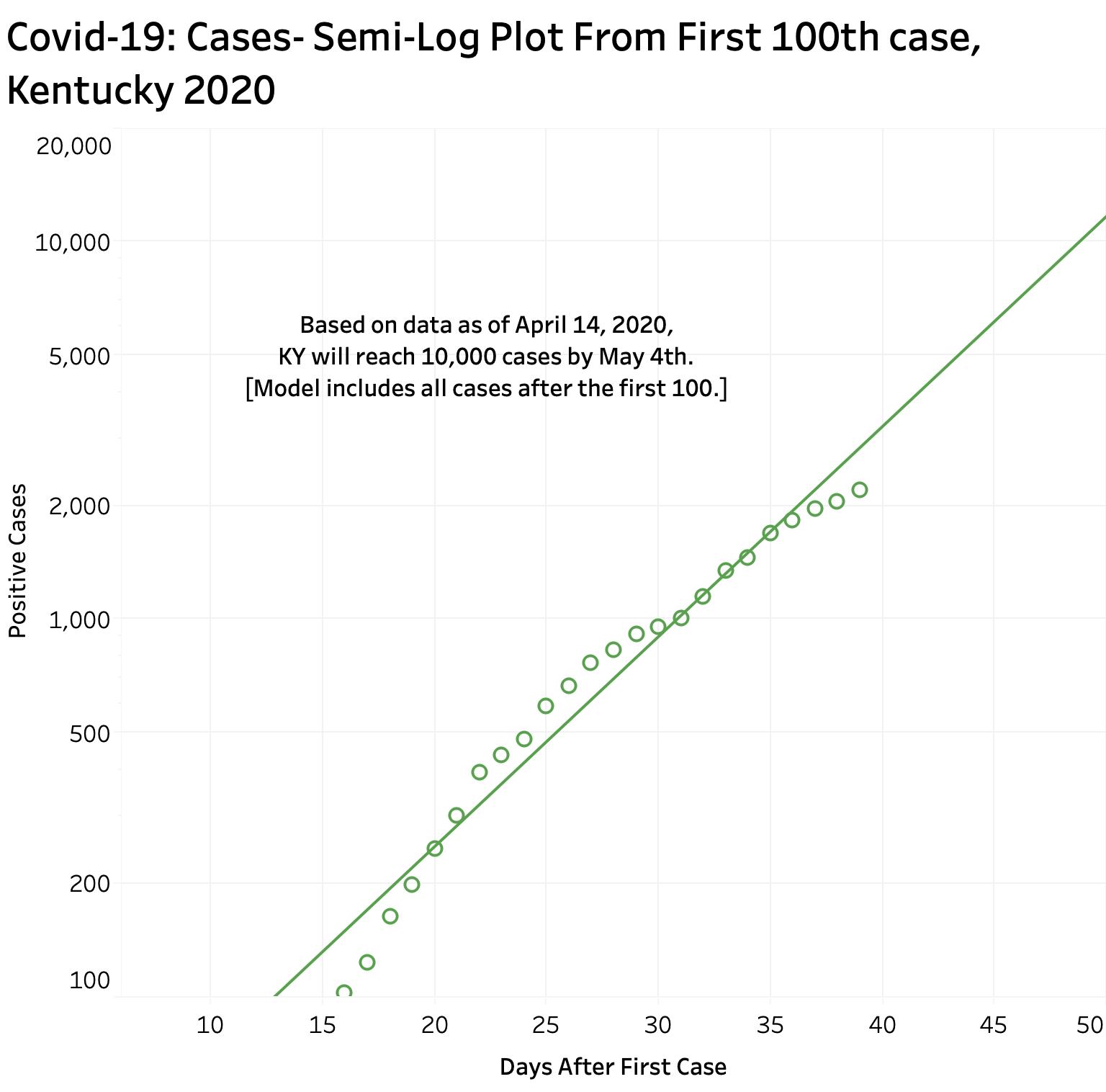
Both new cases and deaths from Covid-19 infection continue to rise sharply in Kentucky. Observed mortality of confirmed cases remains above 5%. Simple daily plots of the numbers of cases by themselves cannot indicate whether we are turning a corner or flattening a curve. Comparison with other states and the nation as a whole does suggest our efforts to mitigate the disease are having an effect. Plotting the data on a logarithmic scale makes visualizing small and large numbers together on the same scale more accessible to analysis. More to the point here, such semi-log plots of the numbers enable us to observe whether the rate of increase in cases or deaths is actually slowing down. Over the past few days, there have been tantalizing suggestions that in fact that both cases and deaths are in fact doing so. Additional reported numbers over the next few days will clarify this hoped-for shift. Nonetheless, we have not achieved plateaus of either daily reported cases or deaths. In fact, semi-log plots of the number of new cases over the 30 days since the 100th new case show continued exponential growth with doubling times of every 5 days. Unless the very recent possible dip in new cases is real, at the current rate of increase, Kentucky will reach 10,000 total cases as early as May 4th. It seems to me that now is not the time to throw in the towel. It is appropriate to begin planning for an eventual data-driven, gradual, and stepwise reversal of our current non-medicinal efforts to deal with this stunningly infectious new disease, but otherwise it’s not very smart to do so precipitously. We have much more to learn about what is happening behind the scenes and our testing capability is still on its baby legs.
Methods.
When Kentucky’s Department of Public Health and Governor Beshear began offering daily reports of the total numbers of new cases and deaths. The data is being collected in the fog of an epidemic and is not perfect. The numbers are presently higher than those reported by The New York Times or Johns Hopkins University– two excellent websites to learn what is happening around the world. I assume our Kentucky data is more current and I use it for this analysis. I prepared data visualizations and used the statistical capabilities of the software package-Tableau. A fuller and interactive presentation of this updated analysis can be viewed on KHPI’s Tableau Public website.
Is it real?
No one is more anxious than I to see a reversal in our illness counts. I am heartened to see a possible tiptoe downwards of the aggregate case numbers from the trend of the past 40 days, but it is discouraging to see continuing exponential increases. I am digging deep into my mathematical and statistical past when I drag out semi-log plots. Others who are pros are doing the same thing. If I have been mistaken or unclear in my analysis or you can offer suggestions on how to do better, please contact me.
What is our goal?
We are not going to drop the new case-rate to zero anytime soon. I believe we will be seeing new cases for the foreseeable future. This is an incredibly infectious agent. It spreads like wildfire in ships, nursing homes, hospitals, religious gatherings– and presumably schoolrooms. (Fortunately, due to prompt action in Kentucky, we have not had to test that latter environment.) Our primary goal at present is mitigation– slowing down the rate of new cases and subsequent deaths. We seek to protect our hospitals and healthcare entities from being overwhelmed, simultaneously protecting those taking care of the sick. It buys us time to learn more about the virus itself, to devise possible treatments and prove they are effective before they become standard of care. Already it is being suggested that there are alternatives to respirators such as a “proning” position for some patients who would have been intubated and placed on mechanical ventilators by ordinary standards. (Who knows we may even learn better ways to take care of nonCovid-19 patients!) Most important, we can buy time to develop and test a vaccine against the virus. That is probably the single most important thing we can do to break the back of this global epidemic.
Waiting for Dr. Salk.
Let me be one of the first to suggest that the example of Dr. Jonas Salk be adopted. In the 1950s, when my parents would not let me go to summer camp for fear of polio, Dr. Salk did not seek a patent for his discovery of an effective vaccine. His philosophy: “Could you patent the sun?’ How different is the ethos of much of our academic community today. It is the federal government that has and will bankroll the science behind a new vaccine. The current predatory pricing system that disturbs or bankrupts so many of us must not be allowed to continue. In fact, when a successful vaccine is found, I suggest that universal, mandatory, and free immunization ought to be the goal!
Testing:
If we as a community even begin to think about loosening up our social distancing and other non-medicinal approaches to dealing with this epidemic, we are going to have to have great confidence in our testing capabilities. This includes available volume capacity, distribution of sites, quality control, reporting, and more. We are still flying this plane by the seat of our pants, trying to keep it in the air without a complete instrument panel. It is not completely unreasonable to think that a Covid-19 survivor might participate in a more openly public capacity if it is safe to do so. We are going to need a robust testing environment to determine if a presumed recovered individual actually had the Covid-19 virus, became immune, and for that matter no longer has the virus anywhere in their system that makes them dangerous to others or themselves. When rules of no-contact are loosened, we will need to monitor the results carefully. It appears that in other countries that have opened up, the number of cases can bounce back. I wish I had the information to say that we are presently up to snuff in this regard.
Our national failure to prepare for testing beginning in January (or earlier) is more than embarrassing. I have only the daily numbers of those tested that were released every evening from Frankford since early April. There are some holes in that data. Timely reporting from labs has been a problem for clinicians also. As more locations and laboratories become available, I assume that timely and accurate totals reported to the state have become correspondingly more complicated. The fact is that rather than the number of tests being reported in Kentucky going up– it is actually trending down. I have to assume this is due to under-reporting to the state. The alternative explanation is unacceptable.
Mortality.
If more laboratories are doing tests now, reporting to Frankfort may be inefficient if not incomplete– especially if only positive cases are reported. I calculate that over the last two reporting days, that 7.5% of all tests were reported as cases. This is higher than the 5-6% over the prior 11 days. These are pretty high numbers for a community-wide screen. I understand that testing is still prioritized to sick people, at-risk patients, and responders/ healthcare workers. The percent of tests that are positive should decrease considerably as the criteria for testing are broadened. This has not happened yet. Actual observed mortality as of yesterday– the percent of cases that have died– is 5.2%.
What does public health mean?
One of the things that surprised me during the Hepatitis -A outbreak of 2 years ago is that the effectiveness of Kentucky’s public Health Department was hindered (to my understanding) by the fact that the state has a number of different local public health agencies that may or not want to take instruction from above, or do not have the funding to do so. One of the things I would ask for as a community as we emerge from this 11th Passover Plague is that the Commonwealth revisit the organization and funding of a maximally effective public health system. I used to write that, “As a society we are no more healthy than the sickest among us,” and now “… than the one standing next to us.” This is going to happen to us again and perhaps even before we get over this one. We need to be ready. If we are going to ask our public to do hard things, we need to give them the support to make it possible. That includes financial and healthcare support.
Racial and Economic Disparities.
There are increasing reports of striking differences in death rates from Covid-19 for black people and other minority groups. When I was a medical student in 1970, I remember being told on the wards that black people were more susceptible to tuberculosis and did more poorly from it than white people. The implication was that the difference was due to the something about the genetics of being black. After all, in bedside and written presentations of clinical cases at that time, the color of a patient was a factual element stated only after a patient’s age and before gender. That presentation protocol and the state of mind behind it was, and still is, a hard habit to break. We must longer can ignore the non-biological and non-medical determinants of healthcare outcomes. As a society, we have red-lined some or our brothers and sisters into a second-class healthcare system.
End Game and Recovery:
What will healthcare look like when we get past this crisis? I hope it will look very different indeed! When my 1998 cohort of health policy fellows in Washington made the rounds of the many offices of people and entities involved in creating and implementing an increasingly inefficient and unfair healthcare system, we joked darkly that the only way that things could possibly change is for the system to melt down so that it could be rebuilt. There is more than a grain of reality to that. At the turn of the last century, I offered a Vision of what healthcare should look like in the next millennium. It has been 20 years now, and as I look back at it, I am hard pressed to see that anything has changed for the better. (I will present this document again later and give readers a change to disagree.) Many are suggesting that our economic structure and employment customs will be quite different after Covid-19. I earnestly hope that will be true for healthcare, but it won’t happen unless we demand it and are willing to support it.
Enough for now. I reserve the right to add commentary to this or continue in a separate article.
Respectfully,
Peter Hasselbacher, MD
Emeritus Professor of Medicine, UofL
President KHPI
15 April 2020