
No Centers designated in Kentucky.
Earlier this week, the Center for Medicare and Medicaid Services (CMS) announced that 35 U.S. hospitals have been designated as Ebola Treatment Centers. More are said to be announced soon. These hospitals were designated by state or local public health officials as having both the physical and staffing capability to care for these very ill patients. The CDC has published interim guidance outlining the capabilities every Ebola treatment center should have. They are pretty rigorous. Certainly not every hospital is up to the clinical demands, including the many Medicare Critical Access Hospitals in rural or small population centers that must by regulation transfer their sicker patients elsewhere. [The CDC website provides an excellent source of information about Ebola virus disease for professionals and laypeople alike.]
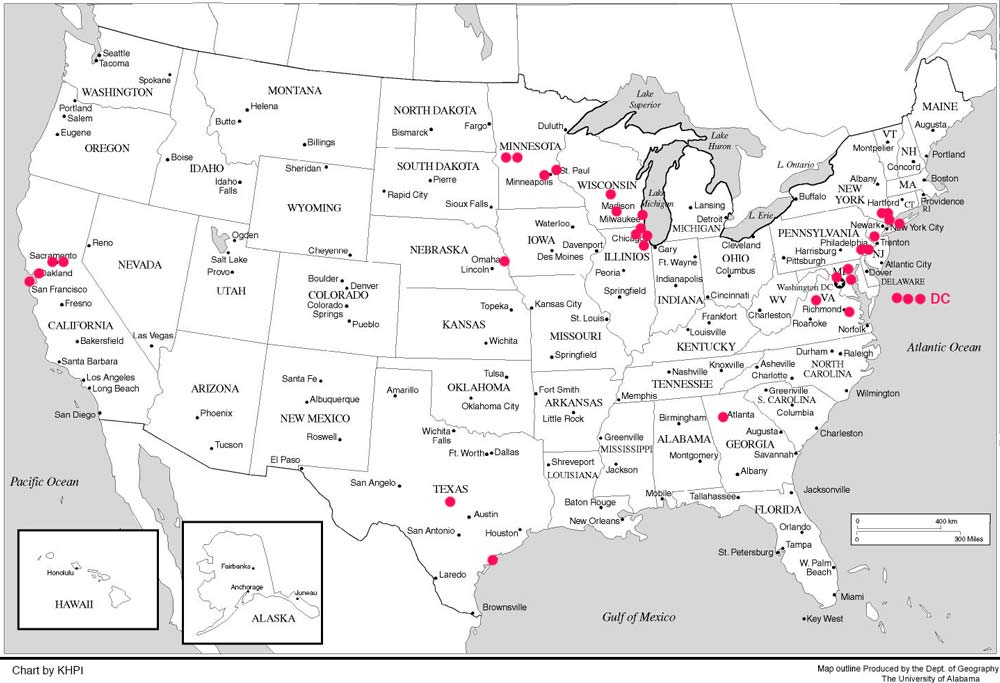
I prepared a map of the locations of these currently designated hospitals All lie within 12 states and the District of Columbia. Chicago and New York City have four each, with three in the District of Columbia. (If I did not immediately know the location of the facility, I placed the red dot under the state name.) There are none in Kentucky. The nearest to us are in Chicago, Charlottesville, Atlanta, and Omaha. All of the 35 that I recognize are major state or private medical school teaching facilities. For the most part, these hospitals are said to be near international airports where individuals from Africa might land, and to be within 200 miles of where 80% of travelers returning from Ebola-stricken countries are currently living. (Emphasis mine.)
I did not expect to see any formally designated Ebola Treatment Centers in Kentucky. Frankly, I am amazed but pleased to see any hospitals at all stepping up to the plate and advertising a willingness to accept these critically ill patients. Not only are they very expensive to care for as individuals, but experience is showing that the presence of an Ebola patient frightens away other patients! I fully expect to see reports of hospitals that have refused to accept ambulances containing febrile patients with even the remotest possibility of having Ebola disease.
Other federal and state initiatives.
Additionally, the CDC has been working with state and local public health officials to identify “Ebola Assessment Hospitals.” These would serve as places to refer individuals who are currently being actively monitored for the presence of Ebola— presumably because of recent travel or patient contact. Treatment of patients at these hospitals could be initiated for up to four days. No such assessment hospitals have been designated yet. In addition to establishing designated treatment and assessment centers, the CDC has established “Ebola Response Teams” made up of multidisciplinary specialists ready to deploy to any hospital with probable Ebola cases.
Good for the goose…
The concept of a “framework for a tiered approach” to deal with the threat of Ebola Virus disease makes good sense, but I would argue that the same conceptual framework should be used for all serious disease! Few, if any healthcare facilities can “do it all.” I worry that the current model of dividing our healthcare system among many nominally independent organizations is a barrier to the coordinated healthcare system we deserve. The right medicine, at the right time, in the right place, and for the right price is what I advocate.
How about Kentucky?
Because the process of treatment center designation is said to a cooperative process with state and local public health agencies, I asked for and received comment from both the Louisville and the Commonwealth public health agencies and from the Kentucky Hospital Association. Certainly our Kentucky hospitals are aware of the risk and have been conducting educational programs and even simulations. The Kentucky Hospital Association is helping to coordinate that process. There are, however, no plans to designate a formal Ebola Treatment Center in Kentucky. It is assumed, arguably, that all acute care hospitals should have or develop the capability to provide initial evaluation and care for suspected patients. If more complex care is needed for a patient with suspected or confirmed Ebola virus disease, the plan is to consult with the CDC concerning the best options for the patient including transfer to another facility.
Should the world revolve around Ebola?
I can’t say this is a bad policy. Recognize, of course, that sick people who do not know what they have or cannot make the trip to Chicago are likely to go to the nearest facility! Every hospital should have the capability of providing at least some isolation for patients suspected of having an infectious disease let alone the big scary E. The reality that so many hospital acquired infections occur every day demonstrates how inadequate or inefficient current hospital practices are in infection control. It must be recognized however, that providing Ebola-level isolation to every patient with a fever is impossible— indeed undesirable. Some balance needs to be made. Not every individual infected with Ebola will get better no matter what we do. More than 1000 individuals in this country are currently being intensively monitored because they had credible exposure to Ebola. I do not know if there are any in Kentucky. In our hyper-mobile world it is unrealistic to assume people will only get sick around international airports. Until the current active epidemic in Africa is brought under control, the risk of new cases arriving in the US or of acquiring their illness at home is ongoing. We will continue, as we should, to bring sick healthcare workers home. We will need to deal with the disease in the U.S. for some time to come.

It is not my intent to inflame unwarranted Ebola-hysteria. There are a lot worse threats to our collective health currently being unaddressed. I wrote earlier about Ebola Virus as a “stress test” to ascertain the health of our public health systems. I do believe, that thinking about and planning for eventualities like Ebola can only improve our overall capability to deal effectively and efficiently with other ever-present illnesses.
There is a medical aphorism that is applied to the process of medical diagnosis— “If you hear hoofbeats in the street, think of horses, not zebras.” That is to say, common things occur commonly. But just as the flesh-and-blood zebras of the Serengeti guide their fellow-traveling wildebeests across crocodile-infested rivers, so we can learn also from the challenge of Ebola. If we can take good care of this disease, we will take better care of everything else.
Peter Hasselbacher, MD
President, KHPI
Emeritus Professor of Medicine, UofL
Dec 4, 2014