
A few days ago I wrote once more about human organ transplantation in Kentucky. No sooner had my bytes hit the ether than a long inked piece featuring the latest hand transplant at Jewish Hospital appeared in the Courier Journal. The article had earmarks of the “press-release” method of media access including a big front page color photo of the surgical suite and the patient. There is no doubt that reattaching limbs to their original owners (or to a new host) represents a spectacular technical accomplishment. Such operations usually make the news somewhere.
Some 70 or so hand transplants have been performed world-wide so far. Immunosuppressive therapy is effective in preventing the majority of the transplanted hands from being rejected immediately, but the risks of side-effects are considerable, especially since hand prostheses work reasonably well for most patients and prosthetic technology is improving rapidly. Postoperative physical therapy is rigorous and lengthly. Sensation returns sooner to the transplanted hand than movement. Since so relatively few hand transplants have been done worldwide, and only a handful in any one center, it is difficult to know how to balance the risks against the benefits, let alone factor in the cost. In the available literature I could find, gains in hand function seemed modest at best but few details are generally provided. For this newest transplant, cells, presumed stem cells, and materials obtained from the patients own fat were injected into the hand before and after transplantation in hopes that the results of the surgery would be improved. I am unaware that this has been tried anywhere else or what the basis was for believing it would help.
Postscript to the newest hand transplant.
I was just about to push the button to publish the above when a second press release from the hospital made it again the C-J front page. The transplanted hand/forearm unfortunately failed and had to be removed. A few additional details were provided. (Presumably the patient had consented to the release of such personal medical information in news or promotional releases.) The surgery was part of a “clinical trial” funded by a US military program. No details are available about the nature of the trial, such as how many patients would be enrolled, or how it would be determined whether or not the new approach was successful. A spokesperson for KentuckyOne Health noted that that “doctors don’t know if the experimental therapy had anything to do with the hand’s failure.” Just so! For all we know, the fat-derived materials made things worse. The patient was thanked for his “pioneering spirit.”
Clinical trials defined.
I am fully supportive of controlled clinical trials to compare new approaches with current ones, or to compare existing practices where it is not known for sure which is better. We need to do many more of these. There are, however, rules in clinical research that include making sure that the study protocol has a reasonable chance to detect a meaningful difference between groups. Trying things on individual patients or in small groups with nothing to compare to usually does not cut the mustard. Additionally it is important that clinical research protocols be reviewed by an independent Institutional Review Board and that fully informed consent be given to and received from the patient. Such standards are increasingly important in the era of expanding commercial research in academic medical centers. It may be argued that someone has to go first, or that desperate circumstances require desperate measures. Fair enough. I would nonetheless offer to patients and physicians alike the advice in 1711 of Alexander Pope— “Be not the first by whom the new are tried, nor yet the last to cast the old aside.” There are consequences to being first or even last.
More data about transplantation in Kentucky.
Since the subject of transplantation in Kentucky has come up again, I will take the opportunity to present other data I am assembling. As it happens, a federally designated organization, United Network for Organ Sharing (UNOS), compiles data from all American transplant centers and makes it available to the public. I made a special request last week for additional information about the insurance status of transplant recipients which is not available on the UNOS website. If I get anything, I will publish the results, but in the meantime, what is already available should be of interest to Kentucky policymakers and citizens alike. I believe that our two academic medical centers need some independent advice from the rest of us.
Kentucky not a transplant Mecca.
In 2013, the most recent year for which full 12-month data is available, 28,954 solid-organ transplants were performed in 46 states, the District of Columbia, and Puerto Rico. (See Excel file.) This is essentially the same number of transplants performed in 2006. I am assuming that the limiting factor is availability of donor organs. There was a bit of a slow-down during the recent recession. In 2013, solid organ transplants were received by 326 individuals in Kentucky at either Jewish Hospital or the University of Kentucky Hospital which are the only two such centers in the state performing adult transplants. (Only a handful of transplants to children younger than 11 are being performed in Kentucky. More about children later.) It is instructive to compare the number of transplants and corresponding national rank with our border states.
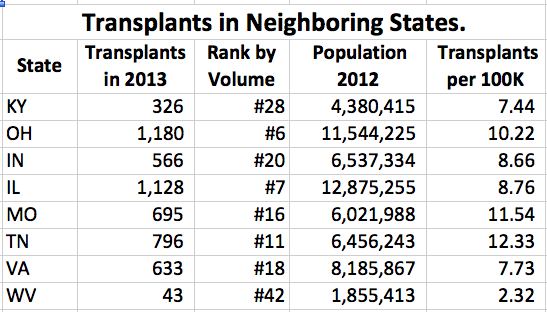
Only in West Virginia are fewer than Kentucky’s 326 transplants performed. In comparison, Ohio and Illinois are ranked in the top 10 nationally in terms of the raw number of transplants performed. Kentucky is ranked #28. Of course the populations of these states vary. Assuming equal access (which seems unlikely), one should anticipate that states with more people would do more transplants in-state. The column on the far right above adjusts the number of transplants for the estimated population of the state in 2012 and is expressed as transplants per 100,000 people. (See Excel file for rate data on all states.) Again, only in West Virginia is the rate of organ transplantation lower than in Kentucky. However, there is another factor that would distort transplant rate— going to another state for the surgery. Thus is it is possible that Kentucky residents are going to Tennessee, Missouri, or Ohio for their transplants. This is certainly the case for pediatric transplants.
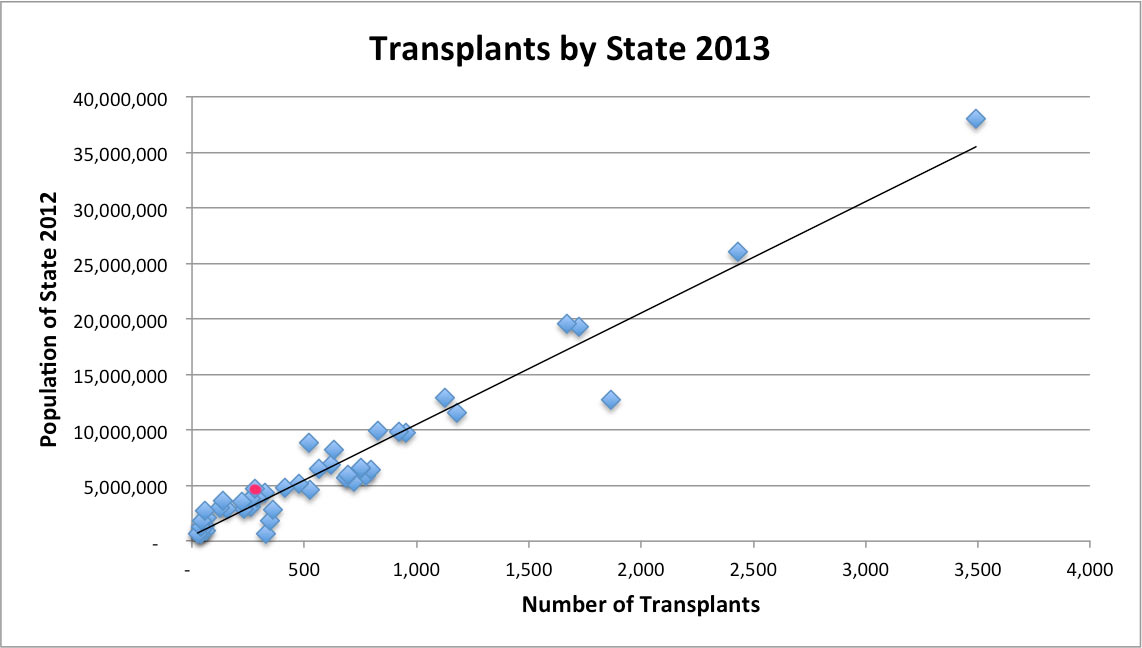
Below is a scatter-graph of state population vs. number of transplants done in a given state in 2013. Kentucky is represented by a red dot. States lying below the line do more transplants than would be predicted based on their population. This is to be expected if for no other reason than that four states have no transplant centers! Additionally, some high profile centers will draw from around the country and the world. Kentucky lies above the line but is clustered with most other states. I would interpret this graph to show that in general the distribution of donated organs in the US is roughly fair if based on population. Kentucky is not far off the line so I would not use this data to claim out of hand that a disproportionate number of adult Kentuckians were going elsewhere for their transplants. It would take more patient-specific information to make that assertion. The data underlying this chart is available here.
Trends within Kentucky- 1998 to 2013.
The total number of transplants in Kentucky rose 19% in the 10 years between 2004 and 2013. This is greater than the 7% increase nationally over the same period. The following graph depicts the total number of solid organ transplants performed at our two Kentucky centers since 1998. (See Excel file for supporting data at these and selected other centers.)
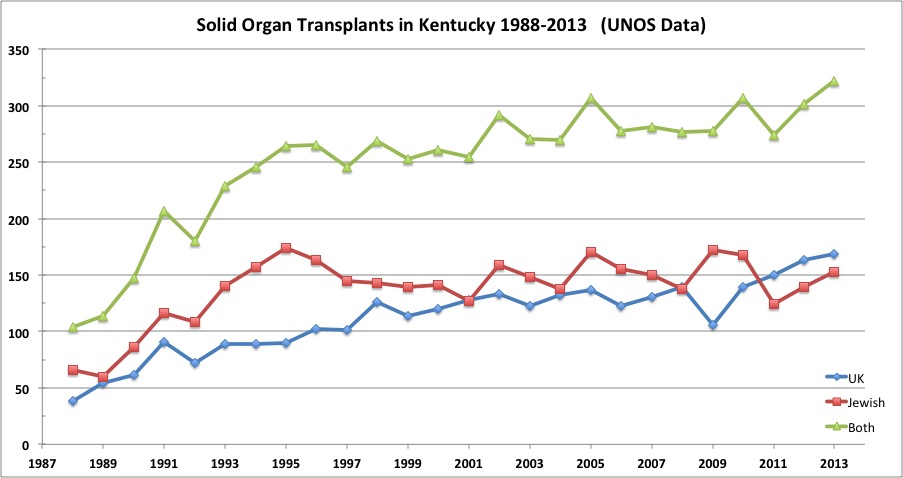
The green line represents the total number of transplants at both centers. Following a rapid rise to 1993, there has been a gradual increase with a slight leveling off during the worst years of the 2008 Recession. The overall increase can be attributed to increasing transplants at UK. We are currently doing more transplants in-state than ever.
University of Kentucky is waxing. Is Jewish waning?
In the earlier years, Jewish Hospital (red line) did a lion’s share of transplants compared to UK. However, little or no growth in the Jewish program has occurred since then. In fact, compared to its peak year in 2009, the total number of transplants there has decreased by 12.4%. Over the same interval, the volume at UK increased 59.4%. Note that the recession year of 2009 was particularly bad for UK which magnifies its increases over the interval examined. Since 2008 the UK increase has been 21.6%— still respectable.
Differences in specific organ volumes.
A breakdown of transplants by organ shows a more nuanced dynamic. Of the six different major organs or combination of organs transplanted in Kentucky between 2009 and 2013, the volumes at Jewish went down for the big-three— kidney, liver, and heart. There was a modest increase in combined kidney/pancreas from 5 to 13, and a five-fold increase in lung from 4 to 19 over the 5-year period. (Details in attached Excel file.)
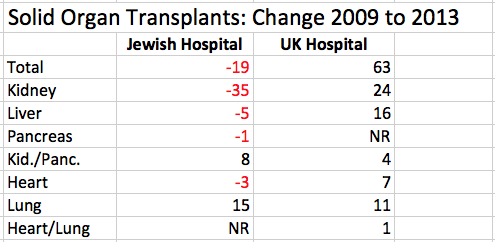
At UK, there were no decreases in transplant volumes compared to 2009 and noteworthy increases in kidney, kidney/pancreas, and lung. (If the base year of 2008 is used, UK dropped 7 livers.) These numbers confirm a communication to me that private nephrologists in Louisville who used to send their kidney transplant patients to Jewish are now sending them to UK with followup care back in Louisville. This seems to be working well. In my opinion this shift is a direct consequence of UofL affiliating exclusively with KentuckyOne and highlighting UofL’s intention to refer patients only to other University or KentuckyOne physicians. I predict we will see more of this recrudescence of town-gown antipathy. Does anyone think this is good?
Miscellaneous transplant facts.
Neither hospital transplants more than one or two pancreases [?pleural of pancreas] yearly, but the kidney/pancreas combination seems to be picking up at Jewish. It appears that lung transplants are on the rise too. Is this because Medicare has expanded coverage for this latter procedure? Perhaps someone in-the-know can explain some of these trends for us. UK has begun transplanting the heart/lung combination which is not performed in Louisville. Of note, Audubon Hospital did a few high profile organ transplants ending in 1989.
Transplant flight?
While it is possible that some adults requiring transplants are going to other states for their surgery, the number of adult transplant patients at the Universe of Cincinnati Hospital in 2013 was 147, fewer than either Jewish or UK. If someone would like to see a chart of transplants over time broken down by organ, let me know and I will tackle it. Children do cross a river.
Transplants in children and young adults.
A handful of children younger than 17 are transplanted at Norton Kosair Children’s Hospital—fewer than 6 in each of last few years, and only 4 in 2013. Jewish does not transplant individuals younger than 18. UK will transplant an occasional child younger than 18, but none younger than 11. UK sends all its youngest and probably some of its older children to Children’s Hospital in Cincinnati which did 67 solid-organ transplants in 2013 for children of all ages and a few adults. Frankly, these referrals are probably in the best interest of Kentucky patients at this time.
What should transplantation in Kentucky look like?
How many transplant programs does Kentucky need or can support? How many patients does it take to keep a transplant surgeon busy, or for a team to maintain proficiency? I am assuming there needs to be more than one of each type of transplant professional per center. (Even the most dedicated doctor, nurse or technician needs to be able to take personal time off!) Is it better to have a single centralized location for the actual surgery with local followup, or should there be two or even more sites throughout the state? Should we farm-out the less frequently performed organ transplants to out-of-state centers with more practice? Why is that not a good idea? I might argue that a center performing only 2 or fewer pancreas transplants per year should not be doing any. Despite the prominence of heart transplant in popular culture, I was surprised to see that each of our two programs do fewer than one heart transplant per month. Is that enough to support two centers? Is it enough to support even one?
I do not have the knowledge or experience to answer these questions definitively, but I do have the right to ask them. Given the apparent animosity among our two major university medical centers and some of their local partners, I do not believe it is appropriate for them to decide by themselves what is best for Kentucky!
As always, if I have made an error of fact or you have a better interpretation, please let me know. You may use the comment function below. You need not enter your name or email if you wish to remain anonymous. Otherwise contact me confidentially through the Blogroll in the sidebar, by email at phasselbacher @ khpi.org, or by phone 502 802-5092. Let me know too if this page or others are not working correctly.
Peter Hasselbacher, MD
President, KHPI
Emeritus Professor of Medicine, UofL
December 2, 2014
I was Chair of Anesthesiology at Jewish Hospital for many years—when we were really active in transplantation. If you don’t do a lot, don’t do any. Also, with the advances in biotechnology, it really does not make much sense to transplant a hand with years of physical therapy, rejection and drug risk, and marginal functional result.