
Is Rome Burning While Nero Fiddles?
 Kentucky’s Hospitals have not done well in the past on national Hospital Rankings including the Leapfrog Hospital Safety Score. Things seem to be getting worse. In the most recent iteration last month, once again Kentucky had fewer ‘A’-rated hospitals than the national median and more hospitals rated near the bottom with increasing numbers of ‘D’s. More troublesome is the observation that 5 of the 6 hospitals receiving a ‘D’ are in the same hospital system. Three of these are in Louisville including two of our major teaching hospitals.
Kentucky’s Hospitals have not done well in the past on national Hospital Rankings including the Leapfrog Hospital Safety Score. Things seem to be getting worse. In the most recent iteration last month, once again Kentucky had fewer ‘A’-rated hospitals than the national median and more hospitals rated near the bottom with increasing numbers of ‘D’s. More troublesome is the observation that 5 of the 6 hospitals receiving a ‘D’ are in the same hospital system. Three of these are in Louisville including two of our major teaching hospitals.
I am not the first to have concerns that the push by payers of medical care to “pay for quality,” based as it is on current measures, may not be ready for prime time. Hospitals are now being penalized for low quality services, readmissions, and other factors related to efficiency and quality. It is starting to hurt. As I type this, Congress is considering a vote to protect some hospitals against such cuts in their important Medicare payments if they serve more than average numbers of indigent patients and those of lower socioeconomic status. Care must be taken that this initiative, lobbied heavily by hospital organizations and their partners in academic medicine, is not interpreted to imply that is it acceptable to provide medical care of lower quality to poor people or in teaching hospitals. The fact that this protection is being considered at all is a tacit admission that our current methods of measuring quality and safety are flawed. It is based on the assumption that socioeconomic status is independently associated with overall poorer outcomes. I believe the association is real, but the reasons for the disparity remain uncertain or ignored.
Can we recognize quality when we see it?
A year or so ago I looked hard at the ways a number of organizations purported to measure the quality or safety of medical care. I found unacceptable variation in a single hospital’s ratings among different raters at the same time, or by the same rater over relatively short intervals. I was troubled by the commercial nature of some of the evaluations. [There is money to be made by licensing the use of good ratings for marketing purposes by both hospitals and raters.] It almost seemed that any hospital could find some organization willing to call it “best.” On the gestalt level, based on my own experience, the scores did not always agree with my expectations or were frankly unbelievable. Other policy experts with more experience than I were saying similar things. Nonetheless, this fabulously expensive system is not going to go away soon. We will have to work with it as it evolves to something better.
What prompted this article.
I recently received notice that the Leapfrog Group was publishing its Spring rating of hospital safety. This influential and credible organization was begun by large employers and their benefit plans that wanted their insurance premium dollars to be put to better use. The ranking uses a combination of measures including Medicare quality items and proprietary ones. Because it has been a while since I took a look, and because of very troublesome things I was hearing about our hospitals in Louisville, I downloaded the current numbers. I was frankly shocked.
Not enough ‘A’s and too many ‘D’s.
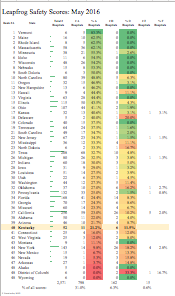
You can take a look at Leapfrog’s own website for the letter scores and the source information behind them. I prepared a summary of the number of hospitals scored in each state together with the number and percent of hospitals with either an ‘A’, or ‘D’. In general, states with a higher number of ‘A’s had lower numbers of ‘D’s but this was not simply an arithmetic offset. I was a little surprised that 31% of all scores were ‘A.’ This seems a little like “grade inflation” to me. Only 15 hospitals got an ‘F.’ (We had one in Kentucky last time.) I also prepared an interactive map labeled with the number of scored hospitals in each state and shaded by the percent of ‘A’s. Hovering over each state reveals the percent of the three scores mentioned above. (Static map here.)
As a whole, Kentucky did not do very well. We are in the lower quartile for ‘A’s and the upper quartile for ‘D’s. Some 21.2% of hospitals received 11 ‘A”s – less than the national 31%. At the other 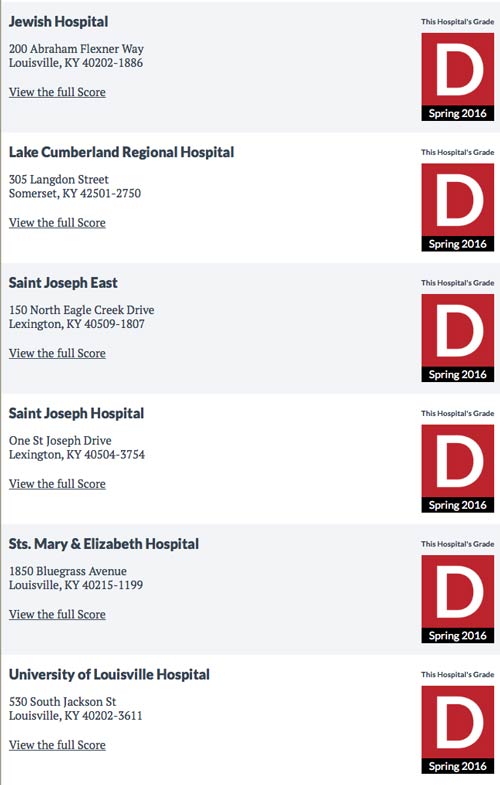 end of the spectrum, 11.5% of our hospitals received a ‘D.’ Most unexpected and disappointing was that not only are there are no “A” hospitals in Louisville, but the city has 3 of the 6 hospitals at the very bottom of the list. The hospitals with ‘D’s were not the small rural hospitals that we are told are in financial trouble, but are major urban hospitals in Louisville, Lexington, and Somerset. Troublingly, 5 of the 6 overall are KentuckyOne Health hospitals including Jewish Hospital, Sts. Mary and Elizabeth, and University Hospitals in Louisville; and the two St. Joseph Hospitals in Lexington. A concentration of low-scoring hospitals in a single system has not happened before to my knowledge. At least two hospitals elsewhere in Kentucky currently working under federal compliance oversight to settle charges of fraudulent billing and quality issues got much better scores than these.
end of the spectrum, 11.5% of our hospitals received a ‘D.’ Most unexpected and disappointing was that not only are there are no “A” hospitals in Louisville, but the city has 3 of the 6 hospitals at the very bottom of the list. The hospitals with ‘D’s were not the small rural hospitals that we are told are in financial trouble, but are major urban hospitals in Louisville, Lexington, and Somerset. Troublingly, 5 of the 6 overall are KentuckyOne Health hospitals including Jewish Hospital, Sts. Mary and Elizabeth, and University Hospitals in Louisville; and the two St. Joseph Hospitals in Lexington. A concentration of low-scoring hospitals in a single system has not happened before to my knowledge. At least two hospitals elsewhere in Kentucky currently working under federal compliance oversight to settle charges of fraudulent billing and quality issues got much better scores than these.
What is going on?
Are any differences in patients served large enough to explain these low scores? Is all quality local, such that large chain hospitals are insufficiently nimble to deal with local situations? Certainly CHI hospitals in some other states like Nebraska did very well with Leapfrog, but Nebraska hospitals did well overall. Other CHI hospitals such as in Texas are in the same ballpark as Kentucky. Is it possible that the layoffs and financial difficulties of KentuckyOne and CHI have begun to effect clinical care? Is the rating system itself worthless? If it is that bad it needs to be thrown out altogether. Don’t you think it is important to know? Because Leapfrog’s quality and safety factors largely track those of Medicare, it is likely that Medicare payments to these hospitals will be cut further. Is that the way to improve the quality of medical care? I wish I knew the answers to these questions.
Many hospitals already excused.
Note that only 52 of Kentucky’s hospitals were rated. The many small Medicare Critical Access Hospitals that primarily serve rural areas are not required to report their quality measures! Go figure. They still receive their cost plus a profit like in the good old days. I am unaware that their Medicare payments are subject to any of the “incentives” that the rest of the Kentucky’s hospitals are. If I were a hospital that had to commit the hugely expensive and manpower-devouring resources to all the reports that regular hospitals are required to submit, I would be unhappy. Is the effort worth it or not? Which hospitals should be excused or protected? Are we on a slippery slope to dismantling the entire quality-evaluating system?
Are there underlying problems?
For all my skepticism, it is difficult for me to dismiss the significance of the low scores. A number of Leapfrog cycles back, University Hospital received a ‘B’. What happened since? I would like to be uncritical or at least neutral, but I have been made aware of increasing reports of major dissatisfaction from senior clinical faculty over the management of University Hospital. Insufficient and inexperienced staffing and lack of understanding of the needs of a tertiary teaching hospital lead the list of complaints. I have been told by several of my colleagues that University Hospital has not been receiving the share of funding it expected from the joint management agreements and that declining funding is impacting the hospital adversely. Faculty are talking openly about the feasibility of unwinding the agreements with KentuckyOne. My readers are aware that I have always thought that the partnership was a bad idea.
Certainly University Hospital is in the middle of a sea change. It was reported yesterday that Ken Marshall, its President for the duration of the partnership with KentuckyOne, is leaving his position. I have always liked and respected him and he is also well thought of by senior clinical faculty. The Department of Obstetrics and Gynecology continues to navigate the impossible (in my opinion) waters between the rules of the Catholic Church and contemporary academic medicine with an interim Chair. The former Executive Vice President for Medical Affairs is currently under federal investigation and out of the picture. Our University President is embattled to say the least, and the Board of Trustees of the University is rendered impotent by lack of action by the Governor for reasons that I cannot fathom. “Rudderless University” are the words that come to my mind as I write this. No matter how capable interim leadership is, it is handicapped by uncertainty and deserving of more attention and support than it is getting.
What happened to the money?
There is little doubt that money is tight if not vanishing at the Hospital. Clinical income should be and was going up because of Kentucky’s healthcare reform– but is the money staying in the hospital? Is money still being drained off for non-clinical uses such as research and general University activities? Is University Hospital revenue being used to pay the debt of CHI or to prop up other KentuckyOne hospitals? The University of Louisville Foundation collects and manages the funds of a number of endowed programs within and without the University. I am reliably told that because of the poor performance of its investments, that the Foundation has told endowed program leadership that their budgets will be unexpectedly and substantially cut from hundreds of thousands to a million dollars each– including the Cancer Center. This is occurring against a background of fabulous executive salaries, “loans” of millions of dollars by the University to the Foundation, expensive ill-conceived legal battles, attempts to raise already unaffordable student tuition, and full-page ads extoling the virtues of President James Ramsey which are ironically silent about what he has wrought at the Medical Center. I am advised that these cuts from the Foundation will damage the Hospital’s academic programs. How can it not hurt its clinical programs as well? This is a time when resources should be flowing into University Hospital, and not drained away to support other institutions or initiatives– or anything else except providing clinical care and medical education. Who will reassure us that this is happening? University Hospital should certainly not be used today as a slush fund to finance research, high executive salaries, or somebody else’s debt. University Trustees who are asked by President Ramsey to raise tuition should be freed from their bondage and allowed to ask what is really going on at the University of Louisville. The principle aspiration of a teaching hospital and Medical School should be to provide the very best medical care in the city. Get that right first. We do not seem to be there yet.
Peter Hasselbacher, MD
Emeritus Professor of Medicine, UofL
7 June 2016
Can anyone offer better news? Have I been mislead? I would like to be accurate.
Dr. Hasselbacher,
Was wondering if you may comment on Dr. Richardson’s timely letter today in the Courier: http://www.courier-journal.com/story/news/local/2016/06/08/surgeon-cuts-make-u-l-hospital-unsafe/85603994/.
Thank you for all you do.
– Concerned UofL Medical Student
Thank you for your kind words.
As I began to write this article 2 weeks ago, I had been informed of the continuing adverse impact of staff and budget cuts at University Hospital and that Mr. Marshall was leaving– although I did not know the circumstances. What I had was a distillation of Drs’ lounge chatter and input from a few former colleagues whose opinions I trusted. I heard yesterday that Dr. Richardson was circulating a critical letter that specifically addressed quality, but I had not yet seen it. After I published my article last night, I too was sent a copy of the full letter. Dr. Richardson has been at the University of Louisville longer than I have, and I have been on its executive faculty for 32 years. His is a senior voice that cannot simply be dismissed by words from KentuckyOne’s public relations office. I have not practiced or taught in the hospital for some time, but I have no doubt that his comments are exactly on target. They confirm what others have been telling me for some time. A precious few senior and similarly loyal faculty had come forward publically earlier. At this time of chaos at the University of Louisville, Dr. Richardson’s comments were badly needed and more than timely. I have not been authorized to reprint Dr. Richardson’ letter, and I am unaware that it has been made public in full. I can tell you that in my opinion, his comments are devastating.
I was glad to learn that Dr. Richardson was dismayed at the resignation of Mr. Marshall, a man who has labored long in the trenches at University Hospital. In fact, I have heard that the word on the street is that Mr. Marshall refused to transfer $10 million from University Hospital to Jewish Hospital. If that is true, it would confirm what I have been told of transfer of resources from University to other KentuckyOne hospitals. (University Hospital is profitable; Jewish Hospital is not.) Indeed, I am informed that even much of the money that has been given to UofL has been in support of UofL Programs that benefited Jewish Hospital as opposed to University Hospital. It should not be difficult to prove or disprove this claim. I would like to think it was wrong.
I was surprised that the University’s official response to to Mr. Wolfson’s article gave considerable credence to Dr. Richardson’s concerns. It’s about time, don’t you think? President Ramsey needs to abandon his attempts to shut down Trustees who have dared to question what is going on at the Medical Center and elsewhere in the University. The sham of what has been orchestrated under the guise of seeking racial balance on the Board is a travesty. The Board is asked to confer degrees on the University’s graduating students and to raise tuition on the next class, but forbidden at the demand of Governor Bevin to exercise its statutory oversight and governance responsibilities. How in the world were Board members forced into accepting this current deal? To my knowledge, as of last week, there is no evidence that the Governor’s office is moving to replace the trustee who resigned in order that a minority trustee replace him.
I must say, there is a lot of blame to go around to have allowed things to go so far. Three years ago at a time of the great fanfare when the management agreement/partnership was signed, and as a sop to those who were critical of the deal, it was promised that the results would be monitored carefully. In my opinion and to our collective shame, most heads looked the other way despite many warnings that things were not right. Whether the contract with KentuckyOne/CHI is unwound or not, it will take years to get us back to where we were in terms of personnel and reputation. Frankly, I do not personally see a way to succeed as an academic tertiary care medical center joined at the hip with KentuckyOne Health. It is past time to part ways. I have already called upon President Ramsey and UofL Foundation Hughes to step down. Their divisive leadership is, in my opinion, destroying the University I knew.
One thing the letter claimed of which I was unaware of is that CHI’s research office in New Jersey has veto power over what research can be done at University Hospital. I wrote previously about KentuckyOne’s attempt to require the UofL Human Experimentation Panel to adopt the Catholic Church’s dogma on contraception and abortion. I had been told that the UofL Research Committee and the Hospital’s Ethics Committee had won that battle. Did they lose the war? I have argued that in signing the agreements with CHI, that in exchange for the promise of contingent research money, President Ramsey’s administration had given away much of the University’s academic, clinical, administrative, financial, and even ethical independence. I seems it also gave away its research independence. What else is left that defines a University?
Surely the matter is fully out in the open now. That is a good thing. The only failure that could be worse is that our community– elected or otherwise– continues to stand idly by.
Peter Hasselbacher