
Reported deaths remain high– predictably so?
With Saturday’s report not yet in, it is clear that daily reported new cases of Covid-19 disease continue to fall sharply. The 14-Day average on Feb 12th of 1989 is lower than any other day since Nov. 13th. The 7-Day Test Positivity rate reported by Frankfort of 6.95 is also falling rapidly and is the lowest since Nov 5th. (See graphic below.) Baring an unexpected high number of new cases tonight, last week will be the 5th week in a row in which cases have fallen progressively. Reflecting the decrease in new cases, hospital and ICU utilization is going down modestly, but hospital utilization remains very irregularly reported day-to-day. All of this is truly good news. However, at the rate of new-case decline since the beginning of 2021, we will not drop below 4-digit daily numbers until the beginning of April. Since what we are doing now in terms of prevention is clearly working, and if we do not slack off as a community, we should be able to do better. However, that will not happen until the reciprocal public health obligations of the individual and their community is recognized and reinforced.
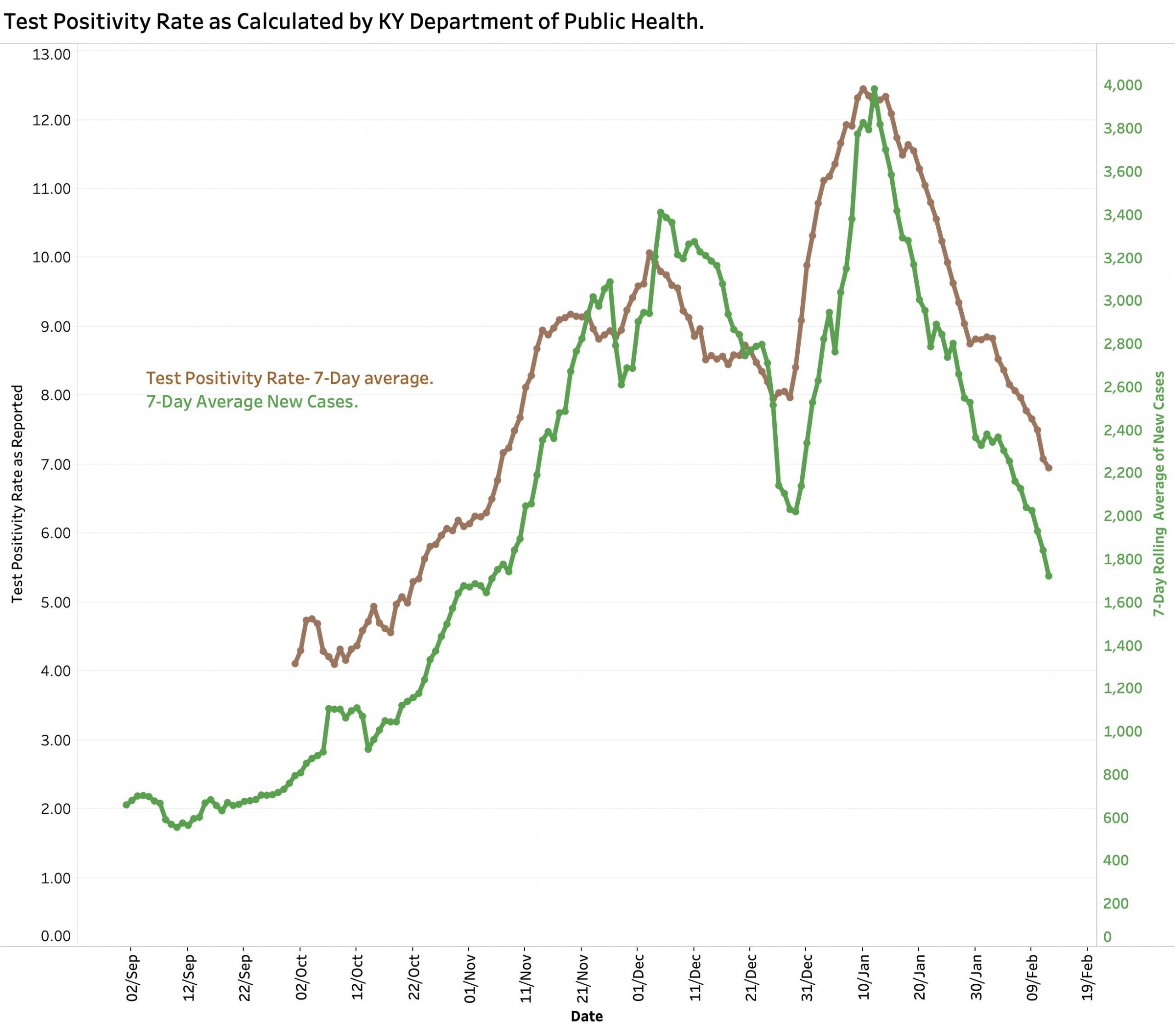
[Note that since by definition all confirmed cases of Covid-19 have a positive test, and reciprocally that having a positive test defines a case, we expect these two numbers to track each other very closely. Recall also that the number of new cases added to the state’s aggregate total of cases have duplicate individuals removed. I do not know if this is the case for the viral RNA tests that the state uses to calculate its Test Positivity Rate. In any event, it is not clear to me that the Positivity Rate tells us any more about the prevalence of disease in the community than raw case counts. Neither represents a random survey of the community. It is generally accepted that large numbers of individuals contract Covid-19 but are not counted because they were asymptomatic, lacked access to a healthcare system, or for any other reason were never tested.]
Deaths.
Yesterday’s 7-Day Average of 42 reported daily deaths, while not as high as the 7-Day Average of 47 on Jan 29th, still hovers in the range of the January and February spike. (The plot of national 7-Day Averages of daily deaths in recent months has the same profile as Kentucky’s numbers as reported by the Wall Street Journal.) There are reasons to expect deaths to lag new cases. Following an initial asymptomatic infection, there is an expected delay in symptoms and diagnostic testing. The great majority of patients who die do so after many days– longer if they are on a respirator. Following death, there is a lengthly chain of procedures related to the collection of vital statistics including post-mortems, preparing and filing death certificates, submitting these to the Public Health Departments, and a final medical review to confirm that the death was the result of Coronavirus infection. Governor Beshear has explained that despite best efforts, the day the deaths are reported may be more than a month later, usually weeks, and certainly not days than the initial infection. [I use this observation to ask again for someone to explain to me why our public health system sits in a world apart from our routine healthcare system, and why the latter is not universal?]
The data and graphics underlying the summary above can be viewed on KHPI’s Tableau Public website. Most of the data visualizations are interactive to some extent. For example, the range of dates for the data presented can be changed by the viewer.
Variant Viral Strains.
Around the world and in the United States mutated strains of the Coronavirus that causes Covid-19 are arising. Some of these result in increased infectiousness that is showing up as rapid expansion in local epidemics. It is not yet completely clear if these strains are more lethal or otherwise harmful to health, or to what extent available vaccines will protect us. In theory, a major lack of correspondence between news cases and deaths could be the result of a more deadly strain. There is no evidence that this is happening in Kentucky at this time. I asked the Kentucky Department of Public Health what we know about the viral strains presently circulating in the state. I am told that we are actively participating with the CDC and other partners to identify individual viral strains. So far, the number of identified Kentucky cases caused by the more virulent UK variant are numbered in the single digits, and that no cases caused by the South African or Brazilian variants have been identified. (These are the three current strains most worrisome on a global basis.) I took this report as good news. Nonetheless, fact that there are any at all means that there are more instances of this strain currently circulating in the state and that the door is open to the others. Surely this is just one more reason why we need to double-down on our collective efforts to simultaneously control the medical and financial implications of this major 21st Century Plague and to get ready for the next one already waiting in the wings!
KHPI and this Covid-19 Update Series.
One of the major authoritative national Covid-19 data aggregators that I and other organizations have been using from the beginning of the Kentucky and national epidemics is closing its ongoing data collection efforts. On March 7, the Covid Tracking Project of the Atlantic magazine, run almost entirely by volunteers, will cease actively collecting new data from individual states and public health agencies. It will maintain and make available their archived data to historians and public health scientists, and even people like me! The Covid Tracking Project took on their role for the same reasons I began to report Kentucky statistics in these pages. There was at the time no effective or reliable source of state or national data from the CDC, FDA or other federal agency. That which was available was tainted by the more-than-perceptible suppression of good science by naked political advantage. Kentucky and its sister states were hung out to dry on their own with little or no federal guidance or support. The federal debacle related to the production of a diagnostic test was worse than no help at all. Collecting and analyzing scientific data is what I did my entire academic career and I wanted to help here at home. I wanted to figure out how to address the question: “How will we know if we are winning?” I believe I have made some contribution to the public discussion but suspect when the Department of Public Health referred to pesky “amateur epidemiologists” they had folks like me in mind. I suspect the folks in Frankfort read these pages. While I had little success in my efforts to communicate with them, I hope they appreciated my global support for their efforts.
Both the Covid-Tracking Project and I are in agreement that under the new Biden administration not only has a page turned, but we are now reading from a new book. Today the CDC has a first-class Covid-tracking website with a comprehensive panel of data and visualizations available to the public. It can do a better job than I can with better data. I recommend that my readers use it as a first port of call. However, to my knowledge, the CDC data is not yet specific to the county or zip-code level which I believe is a critical missing piece that I hope will be remedied. For the county-specific historical data that I have been using I recommend the data-tracking function of the New York Times. There are other data aggregators and reporters that are also reliable. Kentucky Health News does a nice reporting job with a Kentucky focus. Whether these continue to gather their own information individually from hundreds of state and local sources remains to be seen. The obvious most timely and comprehensive information available should be from the CDC. That has not been the case up to now. All state Public Health Agencies report to the CDC. Under the supervision of the CDC, data can be collected from the hundreds if not thousands of state and local public health departments around the country using standard definitions, categories, schedules, and other criteria such that that apples may be compared to apples. Regardless, there will always be a need for more granular local data collection and analysis. Large-population centers like Louisville, Lexington, Northern KY– or for that matter counties– represent the interface between the sick and the rest of us and have the potential to be able to do something effective before the opportunity is lost. If you want to analyze the data in further detail yourself, much of the national and state data subsets can be downloaded as public use files. I wish that Frankfort had provided us with the same advantage.
Proposed Future at LHPI.
My tentative plan is to stop attempting daily updates of the Kentucky data. EWe will see how long I can resist! I will still keep a hand in to continue to try to answer my initial question of whether or not we are winning. There will be specific Covid-related research and public policy issues I will want to address using the new and shiner data. Additionally, I want to recapture some time to continue my research and commentary related to other issues I have been exploring including opioid abuse, the cost of drugs and medical care, the relative lack of value in posting hospital and other charges, the loss of medical privacy, the utility or lack thereof of current measures of medical quality, and any of the many other categories listed in the pull-down “Category” menu at the head of these pages.
I want to thank my readers and those who have reached out to me for information or comment. I hope you will continue to do so. We learn from each other best that way. If there is a request for a specific Covid-related or other issue, I will be glad to test whether any of the current publicly available or even your data can be useful. For now, if asked if we are winning against Covid-19, my answer has to be “we started slow, wobbled some, and have had documented successes– but we have not yet won!
Respectfully,
Peter Hasselbacher, MD
Emeritus Professor of Medicine, UofL
President, Kentucky Health Policy Institute
13 February 2021