
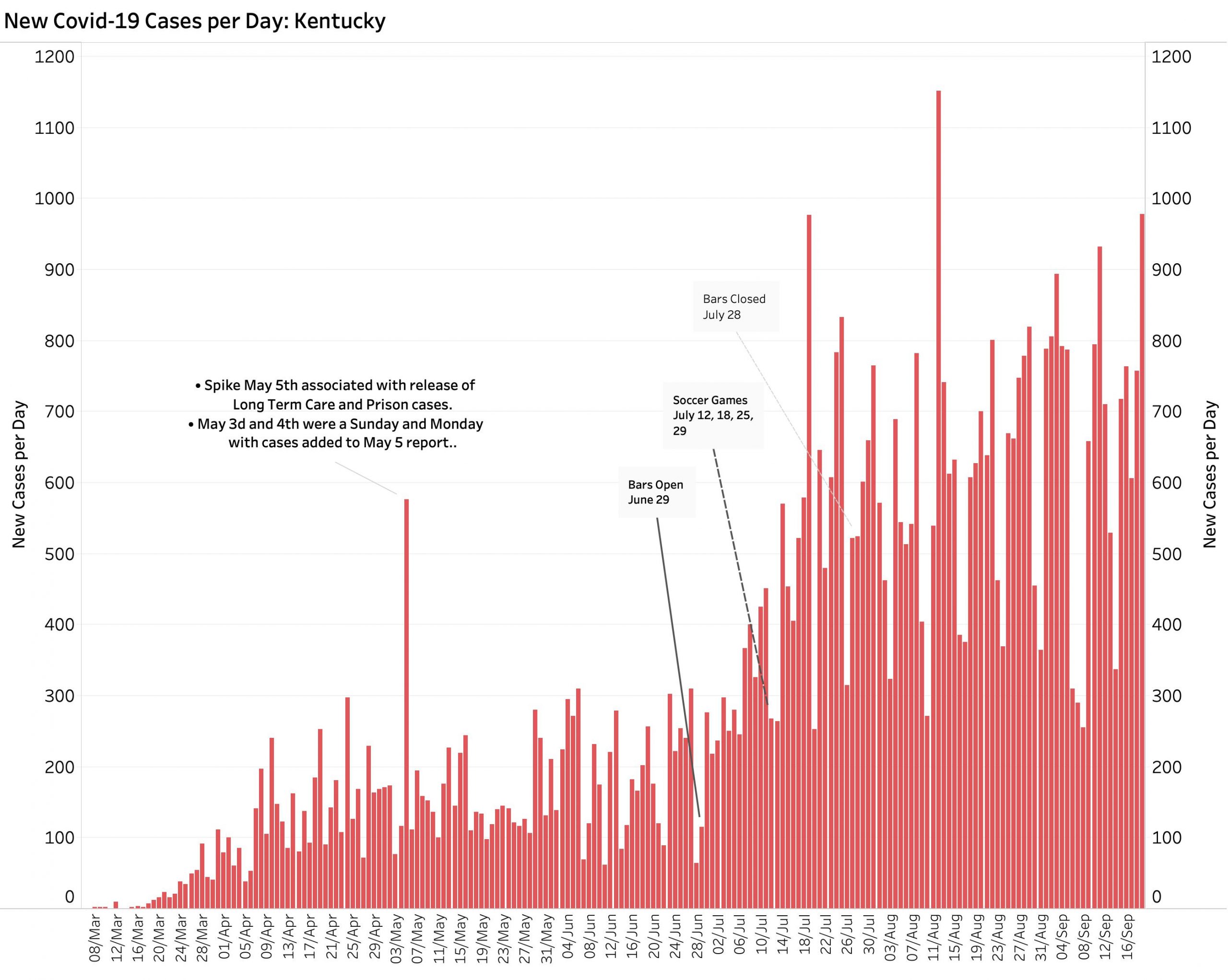
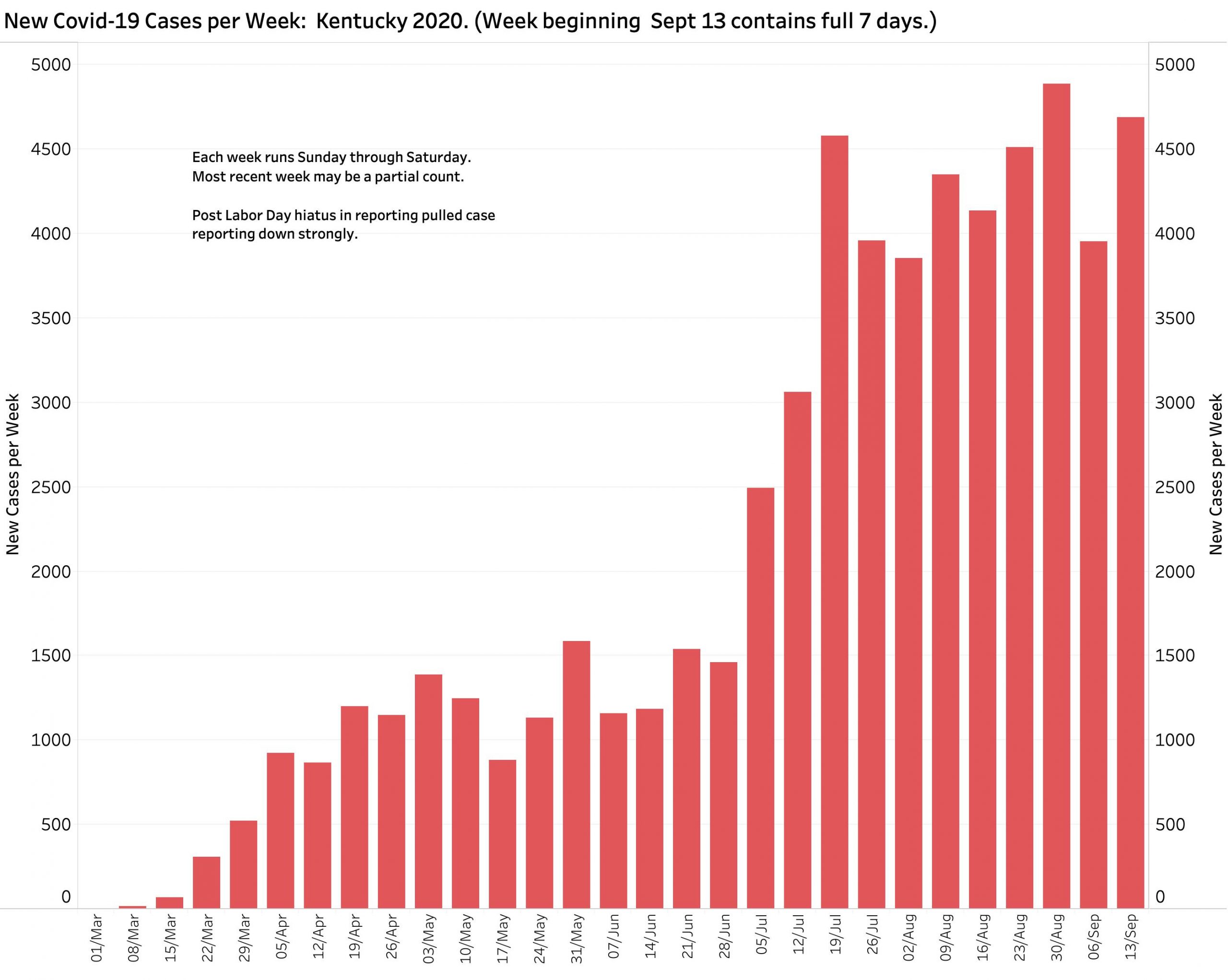
As the week ending September 19 closed, hopes that the number of new Covid-19 cases might actually be decreasing were dashed by Saturday’s 978 new reported cases. The week’s total of 4691 unduplicated new cases was only slightly lower than the previous epidemic high of 4887 two weeks before. Occurring 2 weeks after Labor Day and the Kentucky Derby, it is all too easy to attribute the rising cases to the activities of that holiday period.
Cases.
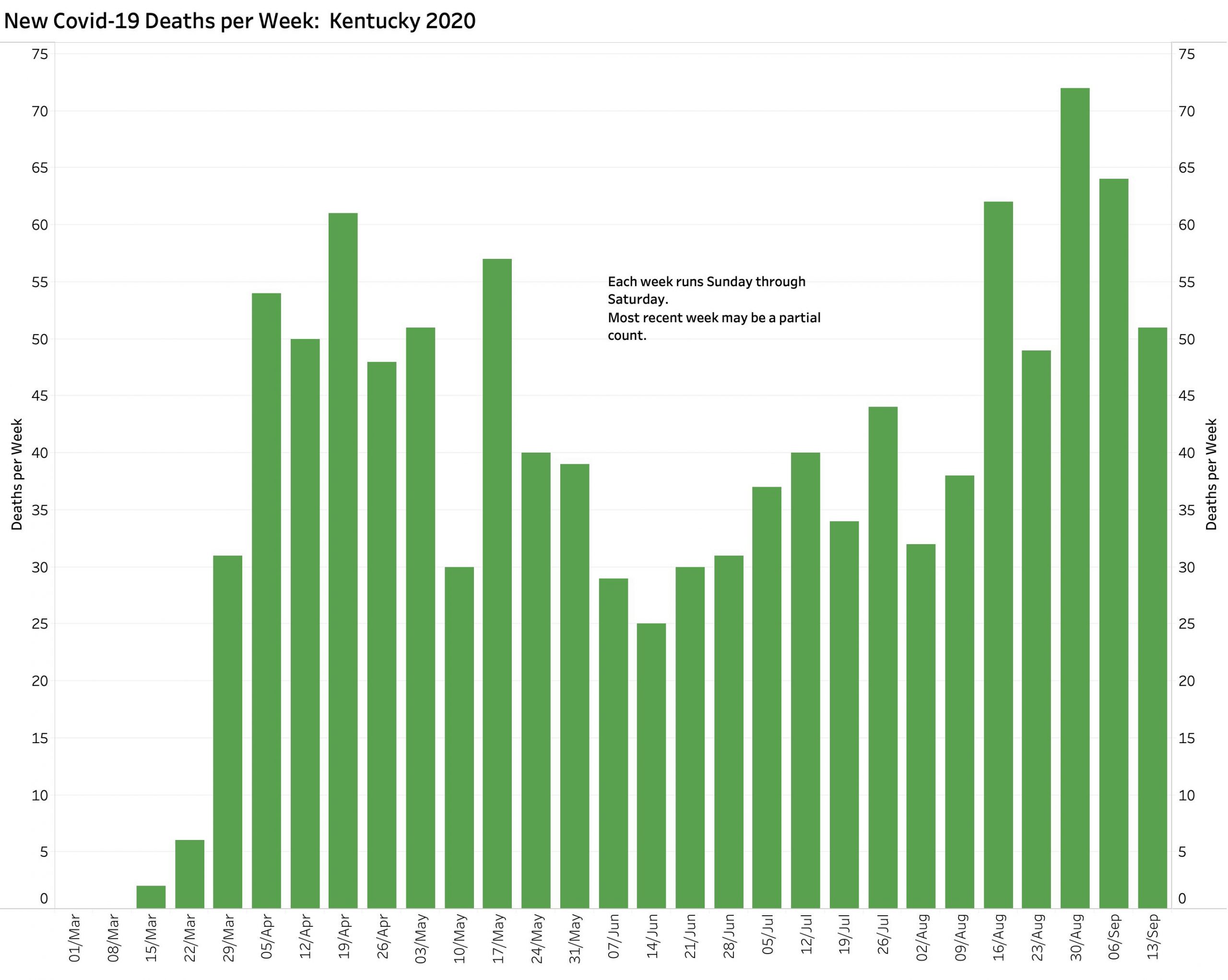
Deaths.
The number of weekly deaths was not as high as the previous two weeks, but deaths can be anticipated to follow the appearances of new cases by some two weeks.
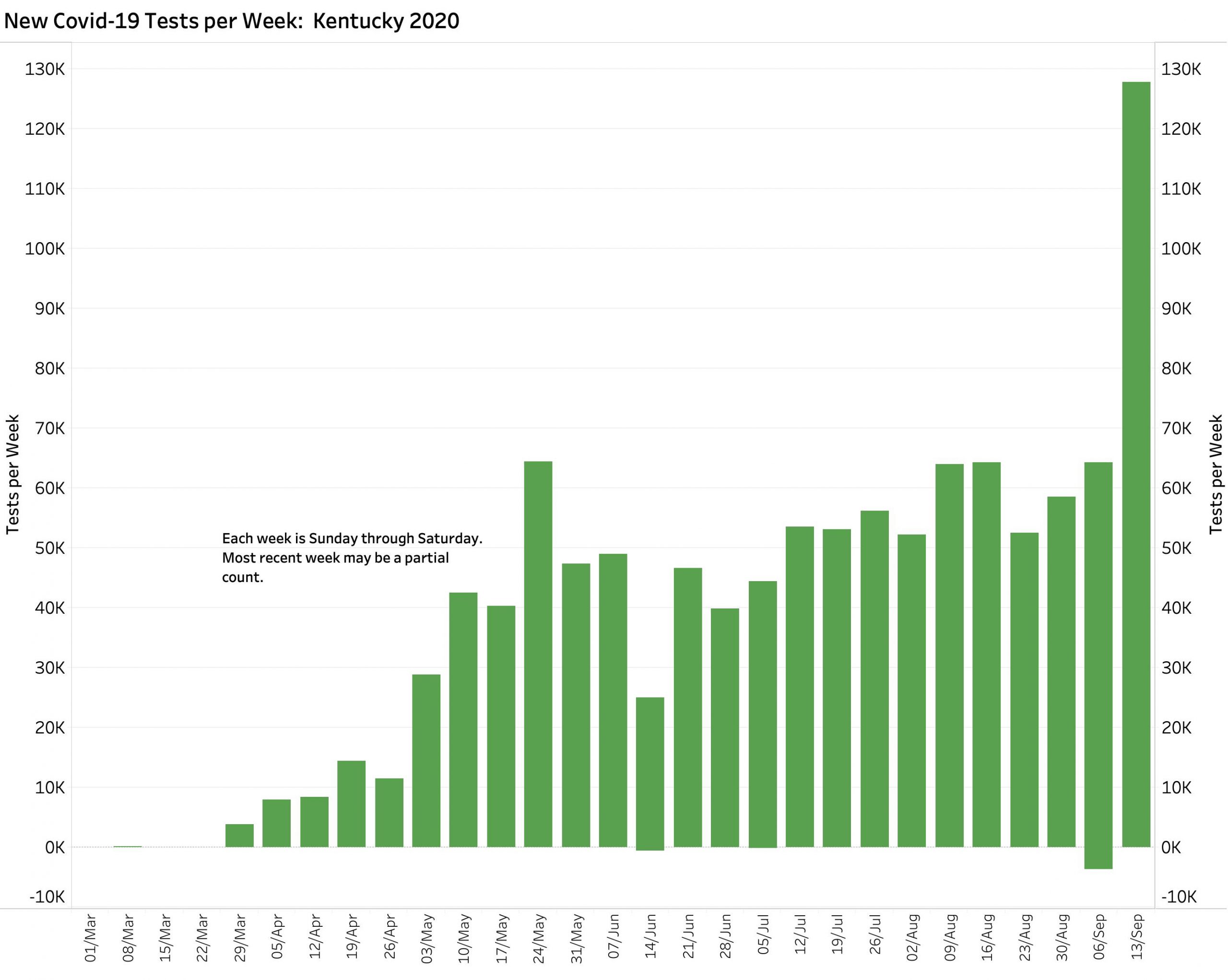
Tests.
The number of new tests reported last week was spectacularly high– double that of any previous week since the onset of testing! Such large variation in both daily and weekly numbers of reported tests is bound to have an effect on the number of cases identified (symptomatic or not) and the calculation of Testing Positivity Rates. I am unable to duplicate the state’s reported Rates from data available to me. I will make another request for details of definition and calculation. Can anyone else help me?
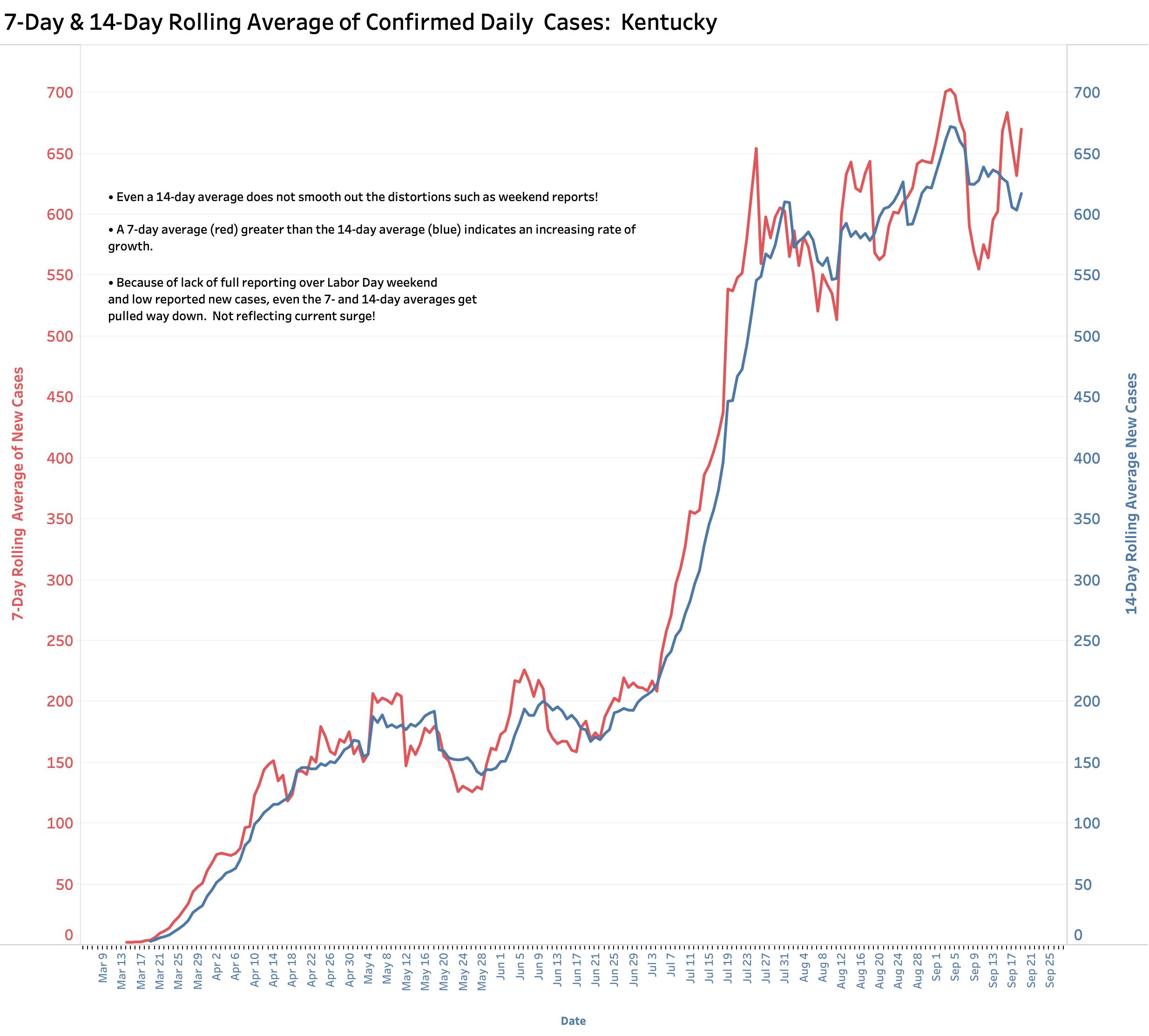
Rolling Averages of Cases.
A comparison of 7-day and 14-day rolling averages of new cases suggests an expanding epidemic in a population that can fairly be characterized as unevenly adhering to recommended health policy interventions. The magnitude of the impact from school openings to the rising incidence of cases has yet to become clear but is clearly a factor. In Kentucky’s current College and University Report Dashboard alone, 35 institutions list 2533 cases of which 1424 are considered “active.” This is obviously an under-report as there are large variations among schools. How are we to explain 1123 active cases at the University of Kentucky against only 11 at the University of Louisville? There are obviously institutional differences in voluntary adherence to reporting requests by the state. Honest transparency is badly needed, now more than ever as schools struggle to simultaneously keep their in-person academic and sports activities open.
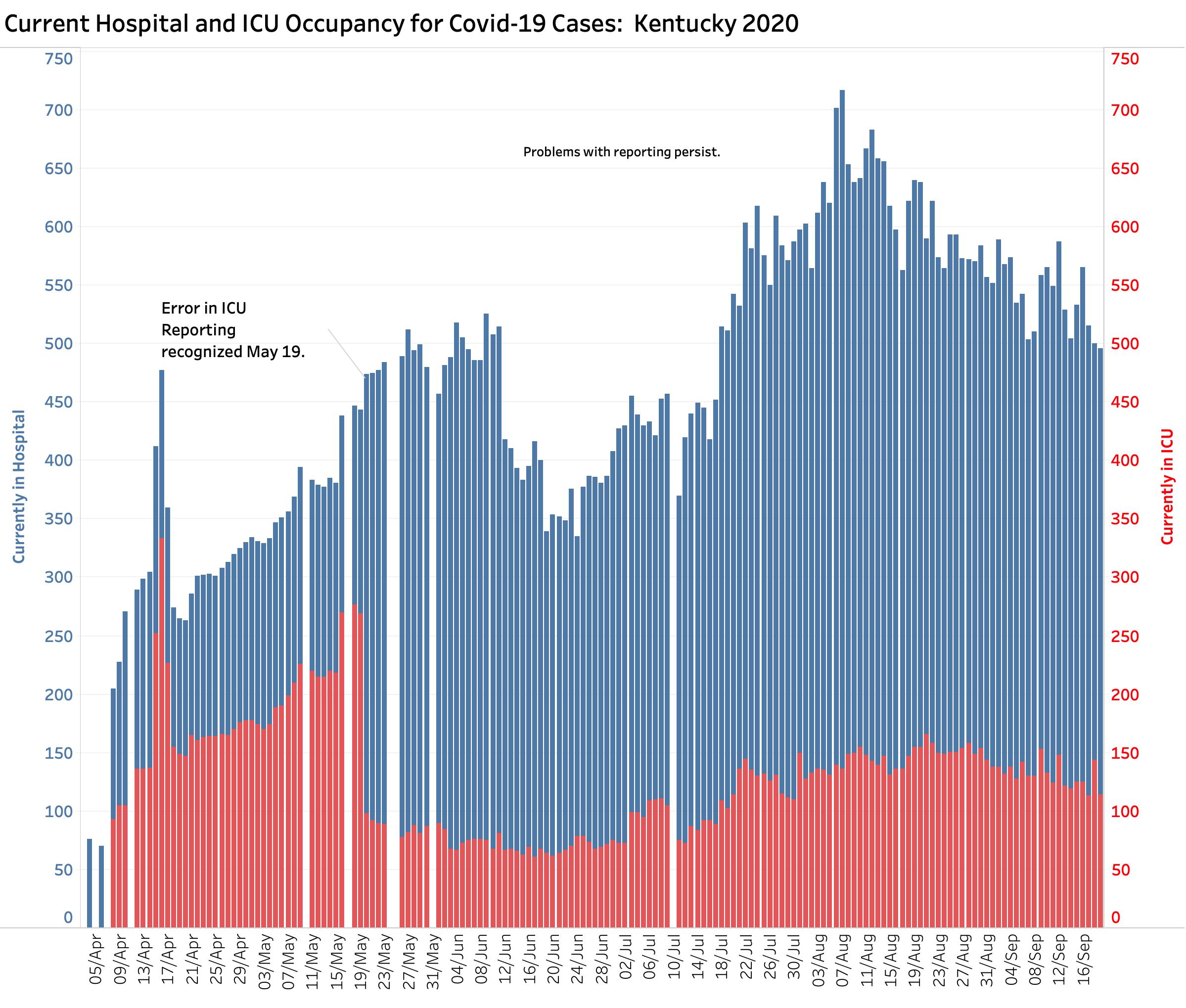
Hospital Utilization:
I do not know how to interpret the available data. Nationally, hospitals are concerned that changes in reporting requirements required by the White House are interfering with the ability to accurately and accountably reflect what is happening in their institutions. In Kentucky, overall hospital and particularly ICU utilization is as high as it has been for a while. In terms of ICU capacity, I cannot comment. Kentucky ICU numbers reported before May 19 were erroneous and cannot serve as a benchmark. Kings Daughters Hospital in Ashland is now reporting that its local surge is overwhelming its capacity– especially for children. No doubt that hospital serves people in multiple counties in Eastern Kentucky where the number of cases has been exploding, and probably also in West Virginia (even though cases in that latter state do not show up in Kentucky’s official case tally).
This is not fake news!
I do not know which troubles me more– the claims by elected and other public figures who tell us that the “media” and “experts” are lying or exaggerating the severity of the Pandemic, or the willingness of a portion of our public to swallow their poison pills. Even in carefully controlled clinical studies, the collection and interpretation of meaningful data is a challenging process. The clinical and other scientists who use such studies have become well acquainted with the pitfalls that must be avoided in drawing conclusions from numbers. Epidemiologists and public health officials are well acquainted with the practical consequences of the infinitely more difficult process of collecting information “from the wild” as it were, where they cannot control the populations for which they are responsible. For legislators and others who complain or seek political gain, I lay our present public health problems at the feet of current and former legislatures who starved our public health organizations of the resources necessary to deal with even their every-day challenges, let alone the predictable episodic challenges we increasingly face.
My readers have seen me struggle to learn how Kentucky’s epidemiologic data can best be used to guide public health policy. In our broadly distributed and semi-independent federal and state public health systems, one expects that numbers will often, if not usually, fail to total to 100%. What is more important it that we have a transparent, definable, dependable, and timely data collection, analytic, and reporting system in place. Can we say that even our every-day health care system meets all those characteristics? Our Commissioner of Public Health, Dr. Steven Stack, is one of the most respected physicians in the nation. He recently served as President of the American Medical Association– hardly a wide-eyed liberal organization. Our Governor Andy Beshear comes across as what we should expect as presidential in his handling of our crisis and his communication with our public. I trust both of them to be acting in our common public interest. Sadly, I can no longer say the same about trusting everything emanating from the White House or the executive branch agencies that it has captured and censors including the Communicable Disease Center and the Food and Drug Administration. I would not want anything that I have written to be interpreted as criticism of our Governor or our state public health officials. My frustration is the lack of just, coordinated, efficient, and effective healthcare or public health systems in either Kentucky or the United States. Any blame ultimately lies with we the people who have not demanded the same.
Plans for this series of articles.
Although I will continue to frequently update the interactive data visualizations that underlie these articles, because of the volatility of daily reports, it does not seem useful to draw conclusions about trends on a day to day basis. Absent a good reason, I will try to focus on weekly changes. I will also simplify the portfolio of interactive data visualizations in KHPI’s Covid-19 Updates on Tableau Public. I initially cast a wide net of possible graphic analyses as I was learning and experimenting. Some of these have not proven to be as useful or predictive as others. For example, my attempt to apply a common method used in Europe to estimate Effective Reproduction Rate (R) was not helpful given the day-to-day variations in a given week. I will continue make the comprehensive panel available separately and use it to explore additional ways of viewing and using available data. I will also keep the Kentucky county-specific epidemiology plots updated because that is where the action is now and where we can learn from each other how to proceed over the next year (or more). I also want to spend some more time catching up on the topics that have interested me over the past few years but have not gone away including our opioid addiction epidemic, the prices of drugs, utilization of medical services, and medical fraud or abuse. I appreciate your attention and support.
Peter Hasselbacher, MD
President, KHPI
Emeritus Professor of Medicine, UofL
20 Sept 2020
We are repeatedly told that large groups tightly bunched together with almost no one wearing masks will result in large numbers of Covid-19 infections. This is what Trump rallies are 3 or 4 times a week. How come I haven’t read one news story about this happening. There are two conclusions. It’s not happening or the news is being suppressed.
There is little doubt that large groups of the college kids partying does result in high numbers of Covid-19 infections. I have always wondered whether alcohol consumption makes an individual more susceptible to catching the virus.
I’m always reminded of the 1971 movie by Dr. Michael Crichton “The Andromeda Strain” in which a military satellite lands in a small town in Arizona and releases a toxic substance that kills everyone except for an alcoholic and a crying baby. It was concluded that both individuals were protected by being alkalotic.
I believe that our approach to virus prevention is way to simplistic and it’s not working. We need to think outside the box.
David O’Reilly