
We were winning for a while, but we have been in this place before.
The last time I posted a Kentucky Covid update in the series was on February 26. Shortly afterwards, both the Kentucky Department of Public Health (KDPH) and the CDC dramatically changed their practices on data collection and reporting. Instead of focusing on the daily counts of new cases, deaths, tests, and hospitalizations, these major public agencies shifted to reporting only weekly summaries an emphasis on hospital utilization. Counting the number of new cases is considered a “back-up” process. Governor Beshear has “paused” giving Covid-19 updates in person to the public. Suffice it to say for now, I no longer have data available or compatible to enter my data analytic and visualization software. It is fair to say that public health experts have expressed considerable concern about the shift in data collection and policy making. I agree and perhaps will have more to say about this later. Last week, based on the KDPH weekly report of April 11, I started preparing this update
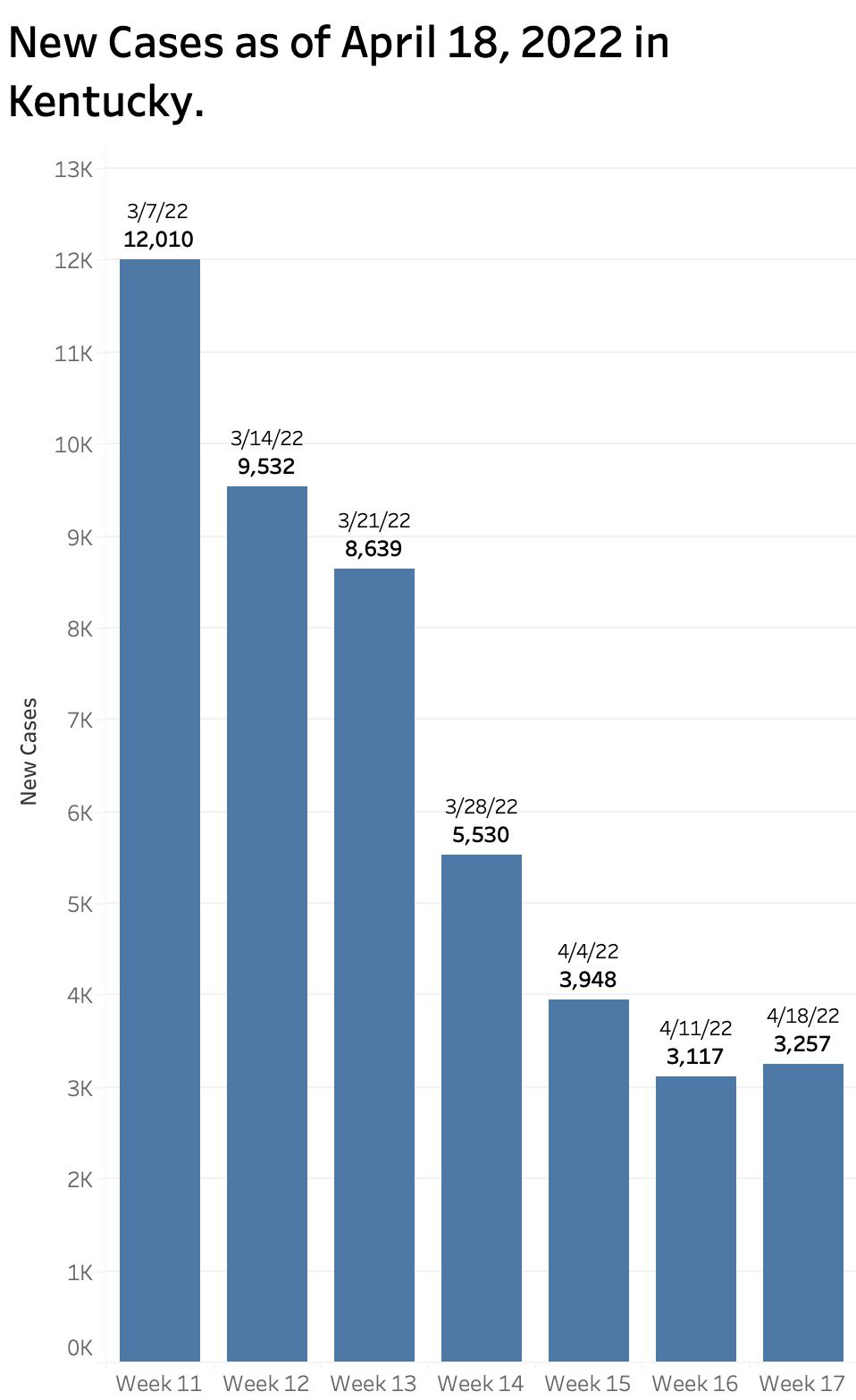
The good news was that over the previous six weeks of reported state data, there had been strong sustained trends downward in the number of recognized new cases of Covid-19 infection and hospitalizations. The number of new weekly cases dropped progressively from 12,010 in the report of March to 3117 reported on April 11. Compare this to the peak Omicron weekly count of over 80,000 at the end of January which was itself more than double the highest count of any previous week of our two-year Kentucky epidemic! Nonetheless, with an average daily count last week of 445 new cases, we were still well above the 7-Day rolling average of 142 in June of 2021 in the interval before the Delta surge when we thought we were finally in the clear!
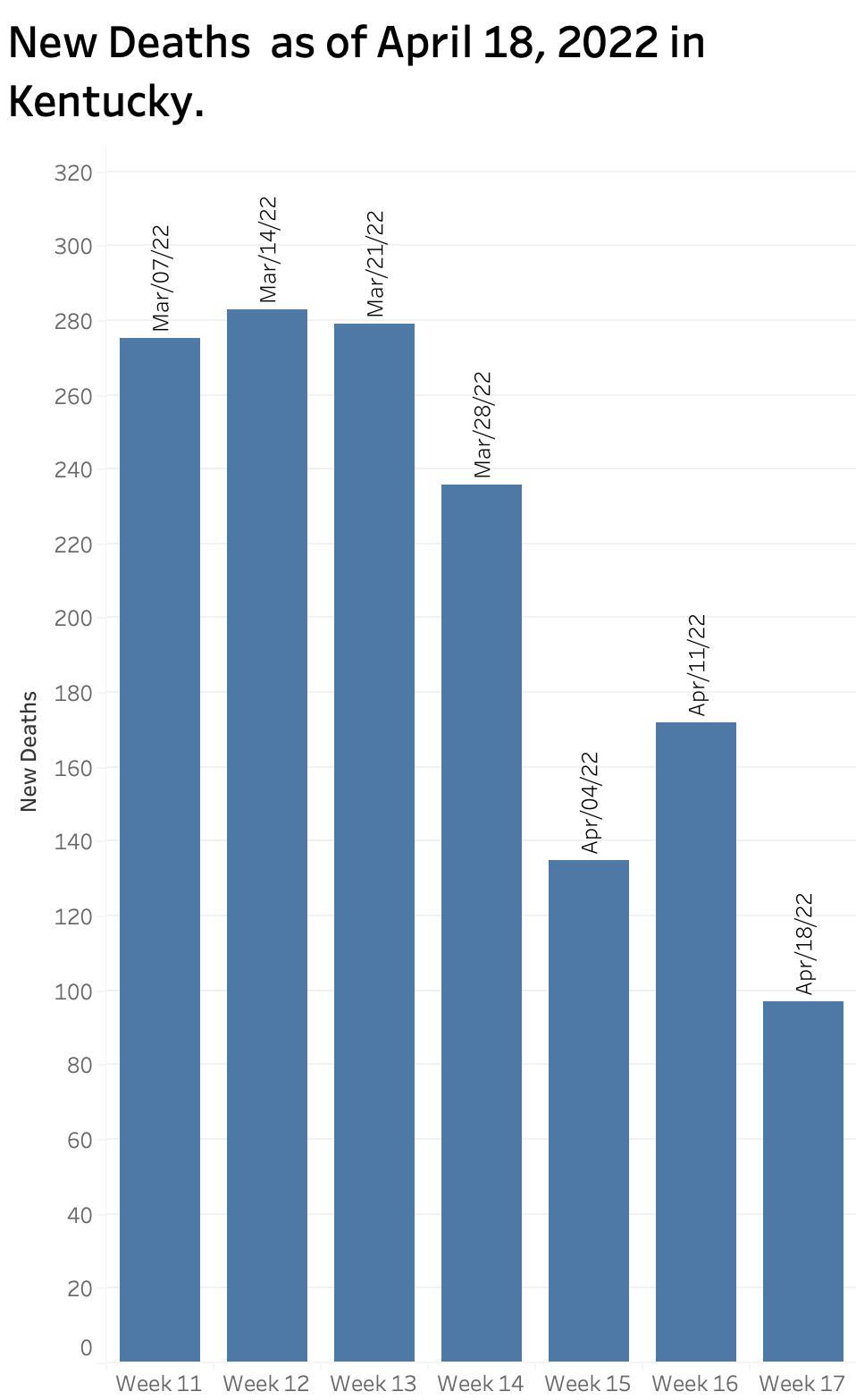
Weekly deaths decreased from 275 in early March to 135 reported April 4 but took a turn upwards to 172 last week. Counts of deaths have always been both erratic and delayed.
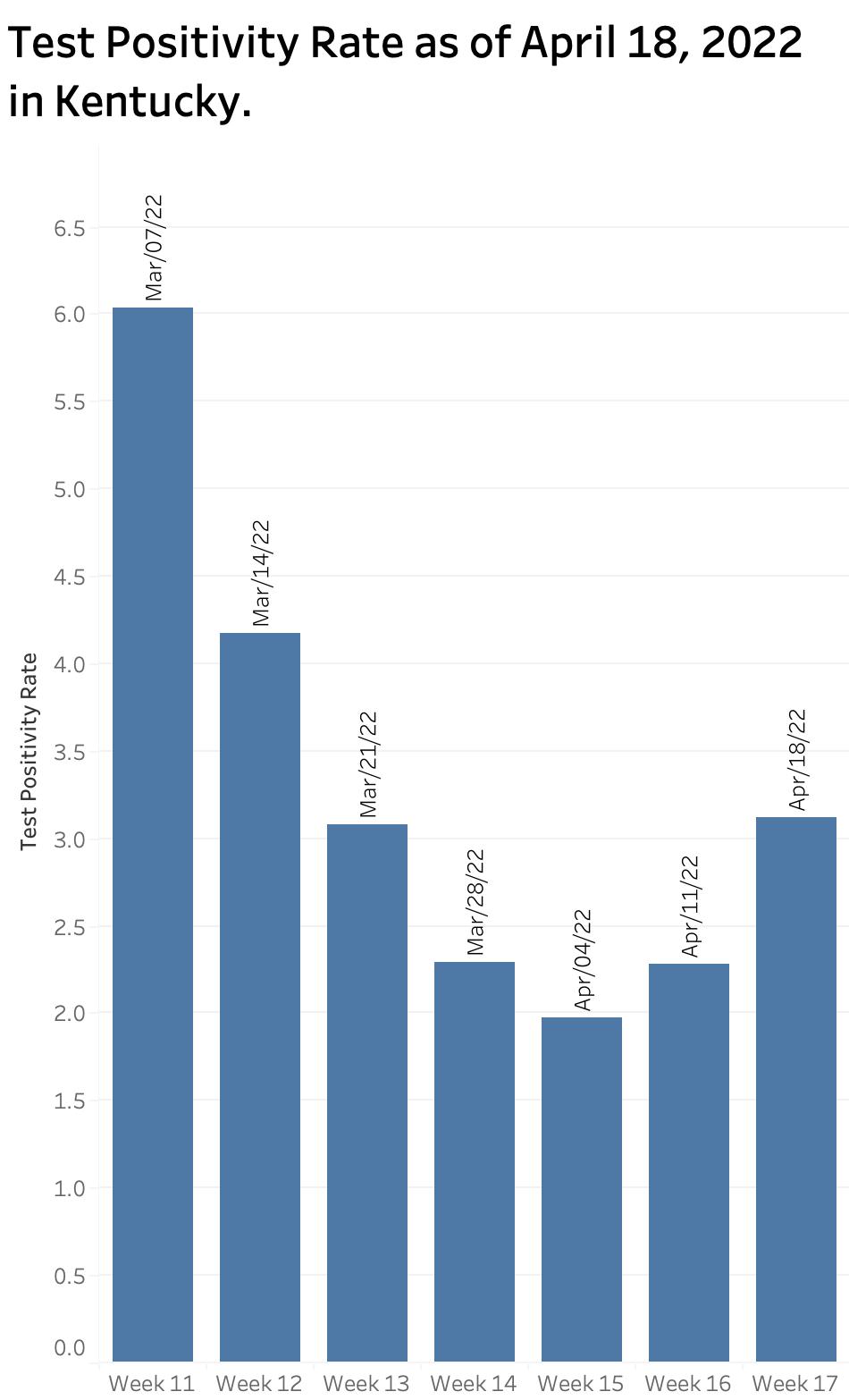
Kentucky’s Test positivity Rate had continued to fall since the March 7 report but took a turn upwards that week from 1.97 to 2.28. The number of PCR tests performed over the last 6 reported weeks also was continuing to fall from 73,786 to 43,773. It must be assumed that a substantial portion of the fall in new cases was due to less traditional laboratory testing and the increasing use of unreported home or office test kits. The proportion of new cases in individuals 18 years old and under continued to hover between 22% and 25% over the 6 weeks of reports.
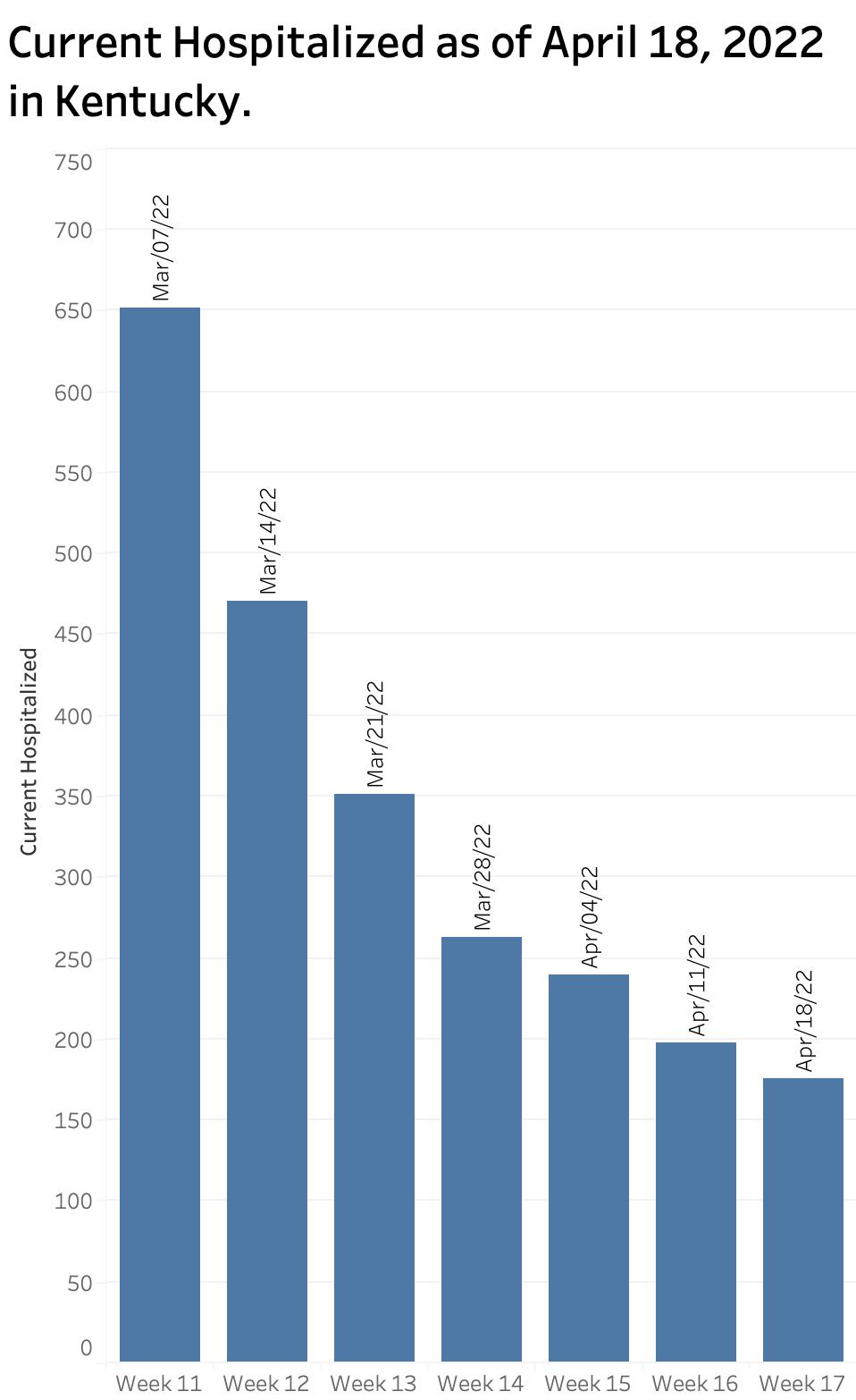
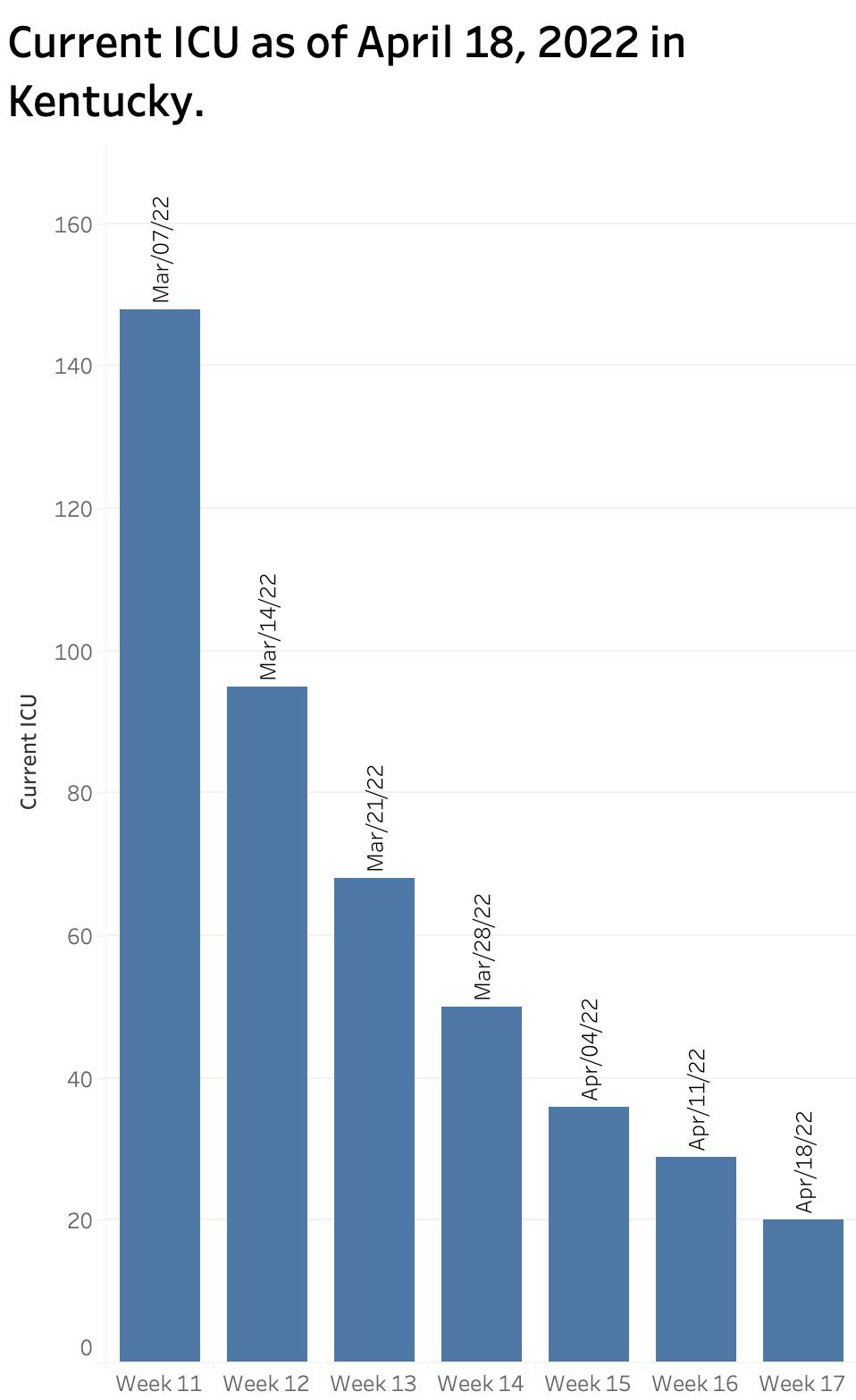
Hospitalization Utilization:
In its once-a-week reports to the public, the KDPH now reports a “Current Covid-19 Hospital Census” for a single day, presumably as of the day of the report. In the report of April 11, the census for Hospitalized, ICU, and “On Ventilator” were 198, 29, and 14 respectively and declining steadily. These numbers were well down from those of the last daily report on March 4 which were 782, 155, and 14.
The discussion above I would have emphasized that the weekly reports reflected the average of 120 individual Kentucky counties and obscured the wide range of the actual distribution of new infections statewide.
Two Different Maps.
Kentucky now offers on its Covid-19 website a map displaying “Kentucky COVID-19 Community Levels by County” produced by the CDC. This stratification is based largely if not entirely on hospital censuses of Covid-19 patients and the availability of beds to care for them. The map last week showed only a single county in the green “low level.” However, when the actual “Incidence Rate” of the number of new cases per 100,000 population is calculated, a very different and more troublesome picture emerges. For example, in last week’s report of the New York Times, of the top 20 counties in the nation with the highest incidence rates, 7 were in Kentucky! Kentucky’s own Current Incidence Rate map had 4 counties with substantial rates, and many more counties with moderate as opposed to low rates. In “hot spot” maps of Covid-19 activity, Kentucky has popped out nationally as a sore toe over the past few weeks!
Weekly report of Monday April 18.
In the busy holiday season that was last week, I never got around to posting the update. I would have summarized our statewide status as being on average in a relatively good place, but would caution that we had been in similar places before over the last two years only to face a rebound of the virus as we relaxed our public health initiatives both personally and collectively. I would have expressed some concern that new Omicron variants were spreading at an ever-faster rates around the world and in in our nation and were quite likely to do so in Kentucky. I would have pointed out that the Test Positivity Rate for Kentucky had begun to rise. Yesterday’s report reinforces my concern that we are on the rebound again. Cases are up in an environment that favors under-reporting. The test positivity rate is higher than it has been in the 4 weeks. I summarize yesterday’s data in the figures below. (KHPI’s data visualization is still online but is current only to March 4, 2022.)
If it seems to my readers that I am unsure what to make of the new national and public reporting initiatives, you would be right. Many things have changed at once and the CDC and the Commonwealth do not always agree in their definitions and methods. What is clear to me is that the parameters I have been tracking daily for the last two years and which allowed credible and timely predictions in the directions we were going are no longer available to me. One of my paths forward is to allow larger and better resourced entities (which somehow still have access to county-specific daily numbers) to carry the ball. I highly recommend the New York Times operation in this regard. The CDC website is also becoming more useful and provides some limited historical data. I anticipate some wrap-up of my Covid experience and concerns going forward with occasional ad-hoc commentaries when I feel I have something to offer. I plan to return to writing about some of other themes of this series which I have neglected but which have not gone away such as opioid abuse and the cost of medical and pharmaceutical utilization.
I wish to thank my readers who have encouraged my efforts.
Peter Hasselbacher, MD
Kentucky Health Policy Institute
April 19, 2022