
[Correction: Because of a systematic error in the on-line database of the Kentucky Hospital Association, the number of angioplasties reported for all hospitals in 2011 was exactly double. This caused me to under-estimate the sharp drop in procedures at St. Joseph London, and erroneously indicated a statewide increase for that year. Corrected charts, tables, and discussion are substituted in the text below.]
The University of Louisville’s new academic and clinical partner, KentuckyOne Health, and its erstwhile suitor, Health Management Associates (HMA), have both been in the news lately but not in a favorable light. A story about HMA was the leadoff feature of the December 2 edition of a 60 Minutes program in which HMA was alleged to have exercised inappropriate and computer-assisted influence over its physicians to admit patients from the emergency rooms of its hospitals who would not otherwise have required inpatient-hospitalization. One of KentuckyOne’s hospitals, St. Joseph London, has been sued and is under federal scrutiny for claims it was performing unnecessary invasive cardiac procedures and worse, operating on patients with normal hearts. For many reasons, these are serious allegations, not least because they impute the ethics and professionalism of the hospital’s management, medical staff, and employees. It would also put human lives at risk without chance of benefit and be be a waste of our collective tax and insurance premium dollars.
Naturally, lawsuits and accusations that have not been adjudicated present only one side of the story. Sadly in this day-and-age, the accusations above cannot be dismissed out-of-hand. I have heard and seen some of the evidence personally and it is both credible and disturbing. The allegations also must be taken seriously because we have all heard them before in other settings. When I was a medical director for a large insurer, I became aware of how consultants with computers were helping hospitals make patients with pneumonia appear sicker than they were in order to obtain the higher reimbursement given for “complicated” pneumonia. One does not have to look hard to find hospitals and doctors that have been found guilty of over-treating the hearts of their patients to capture the disproportionately generous reimbursement awarded to this category of illness. Being a “heart-hospital” is big business for hospitals and doctors– that’s why they are advertised so heavily. Hospitals reward and actually employ doctors who do procedures in their facilities. The financial pressures seem to be too great for some in the healing professions to resist. Others must be looking the other way. Recently in Maryland, St. Joseph Medical Center of Towson agreed to a settlement with the Federal Government, and presumably other plaintiffs, for performing medically unnecessary cardiac procedures. As it happens, that hospital is also a Catholic Health Initiatives hospital, the parent company of KentuckyOne Health.
All of us deserve to know the facts. No one deserves to have to work under such a shadow in a profession for which trust lies at the root of everything we do. It is for this reason that this topic is appropriate for a health policy blog.
Health Management Association.
Of the HMA accusations I know nothing more than what has been in the press. You can watch the 60 minutes program yourself and begin to form your own opinions. The company’s defense that they never tell their physicians what to do is, in my opinion, insufficient.
Actual Data from Kentucky.
To investigate the lawsuit within our own state, I looked at hospital utilization data available on the website of the Kentucky Hospital Association (KHA). It has once again become law that hospitals must post how often they perform and what they charge for some medical procedures so that doctors and the public can make decisions about medical competence and reasonableness. What I found was frankly of concern to me. Sometimes such cases are settled with fines or agreements without admission of wrongdoing. In my opinion, the public deserves to know exactly what happened in London because not knowing, or seeing the hospital fully exonerated, diminishes our trust in the entire hospital and healthcare system of Kentucky.
The KHA makes available the frequency and charges of the 200 most commonly performed services for every individual hospital. For privacy purposes, services that are performed less than 20 times annually are not included. (Would you want to go to a hospital with so little experience in your condition?) I spent several days abstracting the information related to cardiac procedures at St. Joseph London and for Kentucky as a whole. As usual, it is hard to get comparative information about hospitals.
Before presenting some actual numbers, a brief description of how the data is developed may in order. For every patient discharged, a hospital assigns one or more codes from standard sets of diagnosis and medical service categories. This is how the government and insurance companies calculate how much the hospital gets paid for a given patient. These codes are also important for public health purposes. Some codes pay better than others. For example, doing a cardiac catheterization and placing a coronary artery stent in a patient with major co-morbidities and complications (MCC) pays much better than the same procedure on a less-sick patient. For this reason there has always been a cat-and-mouse game of service coding inflation between those who provide medical services and those who pay for them. The KHA website reports medical utilization with the Medical Service Diagnosis Related Group (MSDRG) codes which I use here.
Cardiology Services at St. Joseph London.
With its 78 beds, St. Joseph London (SJL) is the 48th largest hospital in Kentucky– which is to say it is not very big. Yet in 2009, for hospital discharges for Disorders of the Circulatory System (MDC-5), SJL ranked 15th in absolute number of cardiac discharges. The hospital’s average charge for those discharges placed it as 12th highest in the state. Patients with circulatory disorders make up 29% of all SJL hospital discharges, the fourth highest in the state. Only St. Joseph Hospital Lexington, Norton Audubon, and Jewish Hospital had higher proportions of their patients with disorders of the circulatory system. On its face, these numbers would seem to support St. Joseph Hospital London’s emphasis as being a “Heart Hospital.” (Some hospitals are amazingly “Non-heart Hospitals.) “You can download a spreadsheet with all the data here.
I extracted additional details for the most commonly performed cardiac procedures at St. Joseph London and Kentucky as a whole for 2008, the year in which SJL was most busy in this regard. There were 23 separate MSDRG codes related to cardiac procedures appearing in Kentucky’s top 200 for that year. SJL performed more than 20 procedures for each category except one. With respect to discharges of patients having undergone specific invasive cardiac procedures, St. Joseph London again stands with major hospitals, seemingly out of proportion to its size.
MSDRG 247: Cath w Drug-Eluting Stent w/o MCC.
As a specific example, let us look at MSDRG 247, the most commonly performed interventional cardiac procedure at both SJL and in the rest of the state. This discharge category includes patients who undergo percutaneous cardiac catheterization with the placement of an intravascular stent of the drug eluting variety to prop open a presumably critically narrowed coronary artery for patients without major co-morbidities or complications.
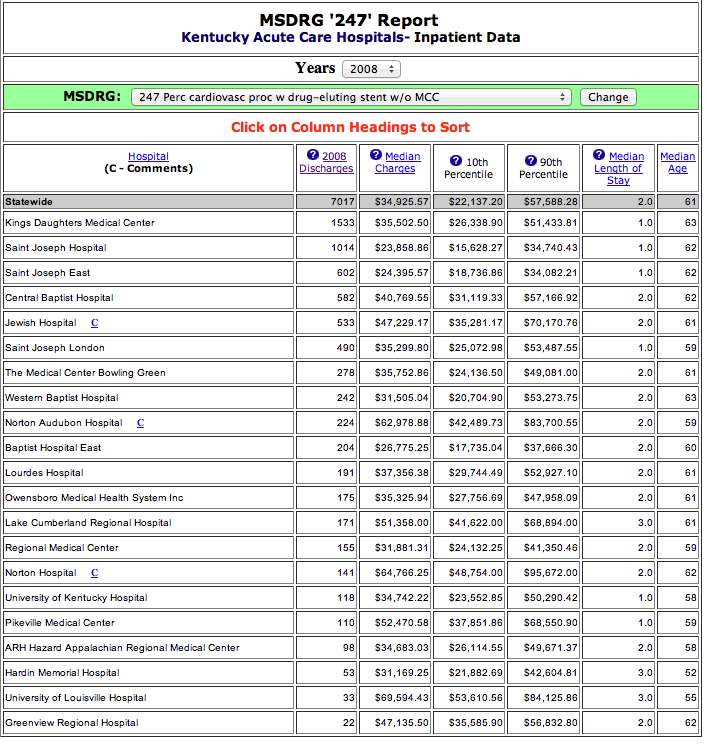
At SJL, this procedure comprises 32% of all its own listed cardiac services compared with 18% for the rest of the state. In 2008, SJL performed 490 such procedures out of a total of 7017 statewide (7%), giving it a rank of 6th out of all 21 Kentucky Hospitals performing 20 or more such caths. For comparison, at Kentucky’s major teaching hospitals, UK and UofL, 118 and 33 procedures were done respectively! Of all 22 different MSDRG services done at SJL for 2008, this is the one that stands out most. Click on the image above for a list of hospitals performing more than 20 of this code annually in 2008.
Even for major cardiac surgery, SJL has impressively high volumes. For MSDRG 233 (Coronary Bypass with Catheterization in patients with Major Comorbidity and Complications) SJL ranks as the state’s 6th busiest hospital out of 14 reporting. Compared to the rest of the state, SJL has more patients with MCC than without which should indicate that their bypass patients are sicker than elsewhere.
Despite the impressive number of procedures, there is evidence that the SJH patients might not have been as sick as elsewhere in the state. Only 11% of the 5 different catheterization procedures listed for SJL had MCC compared to 17.1% statewide. Additionally, while SJL was right up there with larger hospitals for number of catheterization procedures, it ranked comparatively lower for the major cardiovascular surgery that might be expected in a population with so much cardiac disease. Similarly, in the category of Acute Myocardial Infarction with or without MCC, (MSDRGs 280-282), SJL ranked among the lowest listed hospitals in the state. Of course, SJL can argue that it was seeing fewer heart attacks because it was doing so much preventive surgery, but that is not persuasive for me. The other side of that argument is that more patients coming into the hospital with chest pain or cardiac symptoms were having procedures done to them than elsewhere in the state. I encourage others to look at the data (which includes definitions of the MSDRGs) and help us understand what we are seeing. Download Excel file.
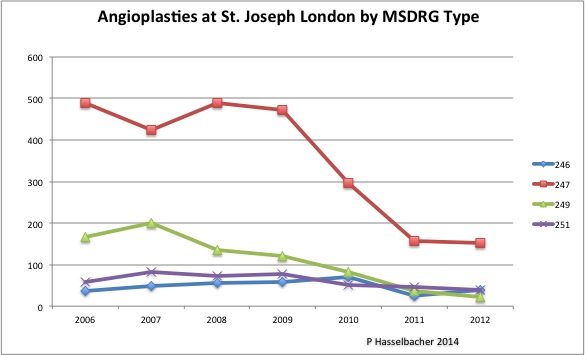
[The chart above includes corrected data for 2011. Click on it for a PDF containing all the data and explanations.]
For me, perhaps the most persuasive evidence that too many cardiac catheterizations with placement of stents might have been performed comes from observing what happened when the hospital came under closer scrutiny from the outside. Between the years of 2008 and 2010 when St. Joseph London attracted outside attention for the appearance of excessive catheterizations and other procedures, there was a one-third drop in the number of such invasive procedures. [Addendum: By 2012, there had been a 67% decrease from 2008. This abrupt drop occurred at the same time that the frequency of these services in the rest of the state as a whole decreased only slightly.] (You can view the data and definitions here.)
Perhaps we will hear an argument that the doctors at St. Joseph London became gun-shy and were under-treating their patients because Big Brother was watching. Such a warning about withholding treatment is commonly offered by those opposed to increased control of prescribed narcotics. I refuse to buy the argument that competent doctors are afraid to do the right thing.
To be fair, another possible explanation of all discussed above is that the healthcare data are so inconsistently collected and of such poor quality that they are worthless. [Addendum: Indeed, the data from 2011 were faulty, causing me to underestimate the precipitous decline in the rates of angioplasty at St. Joseph London!] Since healthcare reform is depending more and more on such quality, frequency, and cost data, this latter explanation is frightening in its own right. As always, I invite readers to comment and assist or correct our understanding. I also suggest that regulators should be looking over more shoulders and I would use such lists to guide the process!
Why are these matters relevant to Louisville and this Health Policy Blog? I offer at least two justifications.
Trust is everything.
We are bombarded by advertising attempting to persuade us to go to one hospital or another to take care of our cardiac, cancer, or back pain needs. The simple reason is that the way our medical system is set up, some services have higher reimbursement than others. Any primary care doctor will back me up on this! It does not help that some diagnoses such as heart attack and cancer, serious as they are, are over-marketed to the point of frightening us into over-treatment. After all, we could die! Shouldn’t everything possible– anything possible be done? Isn’t more always better? Does it make any difference if the treatment has been shown to be helpful or not? If nothing else, the series of articles in this blog has sought to make the point that it is just as dangerous to be overtreated as to be undertreated. If such overtreatment is driven by the bottom line of an office or institution rather than what is in the best interest of people with illness, we will have suffered a colossal failure of our health policy, of our responsibility to each other, and perhaps worst of all, a collapse of the essential trust that is expected of our healthcare professionals and institutions. In my view, that is what is happening.
The $1 Billion is not yet in the bank.
The University of Louisville may have dodged one bullet by not partnering with HMA, but seems now to be joined at the hip with KentuckyOne Health. Its credibility and success will only be as good as that of its partners. Much money has been promised to the University for both patient care and non-clinical purposes. What has not been emphasized to the public, but which is carefully outlined in even the precious few documents that have been made public, is that the big money will appear only if KentuckyOne and the University achieve certain financial and performance targets. Some of these are quite specific. For example, some of UofL’s money is contingent on St. Joseph London achieving a trauma center designation for its emergency room! It is beyond my pay-grade to understand why UofL would agree to such a thing but it is an example of how the money that UofL has touted as a justification for its partnership is dependent on the future financial health of KentuckyOne.
If the allegations against St. Joseph London prove to be true, then there are hundreds, if not thousands of patients with a potential claim for damages from that one facility. I suspect that KentuckyOne Health self-insures its hospitals. It is quite possible that claims such as these can bring KentuckyOne Health to its financial knees and therefore limit the payments to the University of Louisville that the public was promised. The University promised many things to convince the Governor and other state officials to accept what appears to me to be the same deal it offered one long year ago. I hope the University did not promise things over which it had no control.
Peter Hasselbacher, MD
President, KHPI
Emeritus Professor of Medicine, UofL
Dec 20, 2012