
Our body politic is tired of dealing with COVID-19 and has been for some time. The push-back from so many directions, the effectiveness of a variety of both medicinal and non-medicinal interventions, and the reality that a majority of us (including me) have already been infected by existing strains of the causative virus has led us to a posture of dialing back virtually all disease mitigating measures. This change in approach showed up “officially” in a revised set of relaxed recommendations from the CDC related to fundamental public health measures including masking, testing, isolation, and the like. All this in the face of the facts that people are still getting sick, still entering hospitals, and still dying. The fact is that in a world where Covid-19 is perceived to be part of the woodwork of society, there is a level of disease mortality and morbidity that we implicitly accept. The same tradeoffs of benefit against harm exist across virtually any other public policy or individual decisions we make.
Our Current Posture:
Is Kentucky – the “United we stand, divided we fall” state – making the right Covid choices? That we are divided in so many ways is not a matter of debate. Readers of these articles will appreciate that I and others have significant reservations on how we as a state or nation have handled the current epidemic or on our ability to handle other contemporary or the inevitable future public health issues we face. Kentucky is among the states with a “do nothing” legislature. I think it is showing.
Kentucky as a Covid hotspot.
The New York Times has one of the better Covid-19 update scoreboards. Somehow, it still manages to publish daily county-specific counts of cases, deaths, hospitalizations, immunizations, and other relevant information. As of yesterday, Kentucky was not in a good place. We lead the nation with an average daily recent case incidence of 55 per 100K, behind only Puerto Rico and Guam. Our daily average hospitalizations put us at #6. In a map of disease “hot spots,’ Kentucky stands out like a sore thumb. In a listing of daily new-case incidence rates for all US counties, the top 4 are in Kentucky as are 9 of the top 20. Even before the disastrous recent floods in southeast Kentucky, those counties as a group had the highest burden of new cases in the state. The social and economic disruption resulting from the flood puts those folks at even higher risk of illness of all sorts.
While it can be argued that matters are “stabilizing” or even declining nationally, we are currently within the ranges of the previous two years that were deemed unacceptable. Hospitalizations and deaths continue to rise, albeit slowly. Data collection, never optimal, has deteriorated in completeness and timeliness. I do not know what to make of Kentucky’s own home-grown date collection. Since March of this year, Kentucky updates its Covid-19 data only once a week on Mondays and does not provide a state-wide county or date-specific database available for independent public analysis. I have been doing the best I can for this series of articles by combining each weekly report into an Excel file that I make available here. An initial look at this week’s Kentucky numbers may indicate that we have stabilized over the past 4 weeks, it certainly cannot yet be said that things are trending better and the limitations of our ability to capture accurate and timely information become even more apparent. I present some graphic updates below.
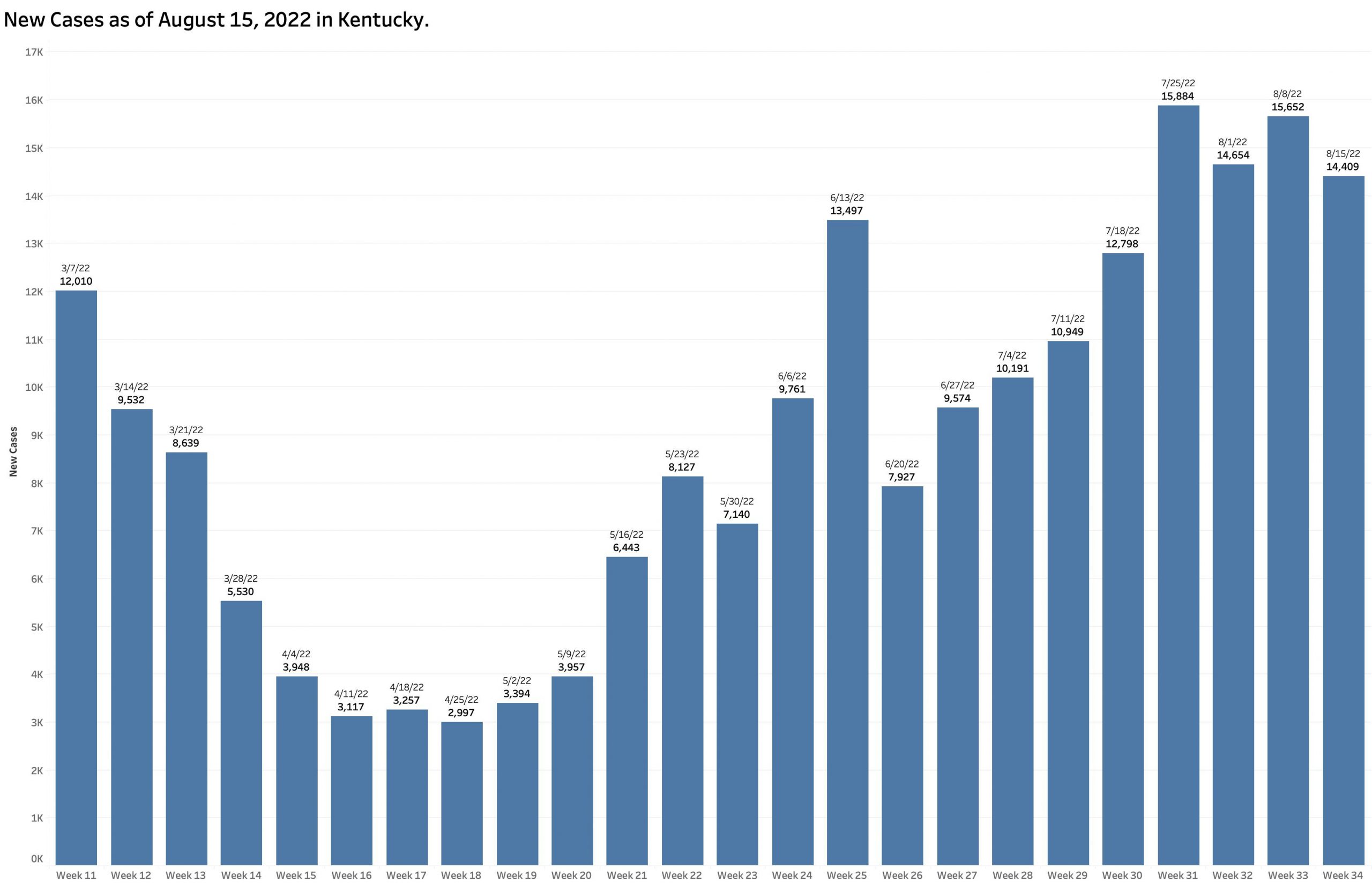
New Cases:
In its report of August 15, the state posted a weekly count of new cases of 14,409. This new case number has hovered around 15,000 per week for the past 4 weeks. For the past week, this translates to an average of 2058 new cases daily.
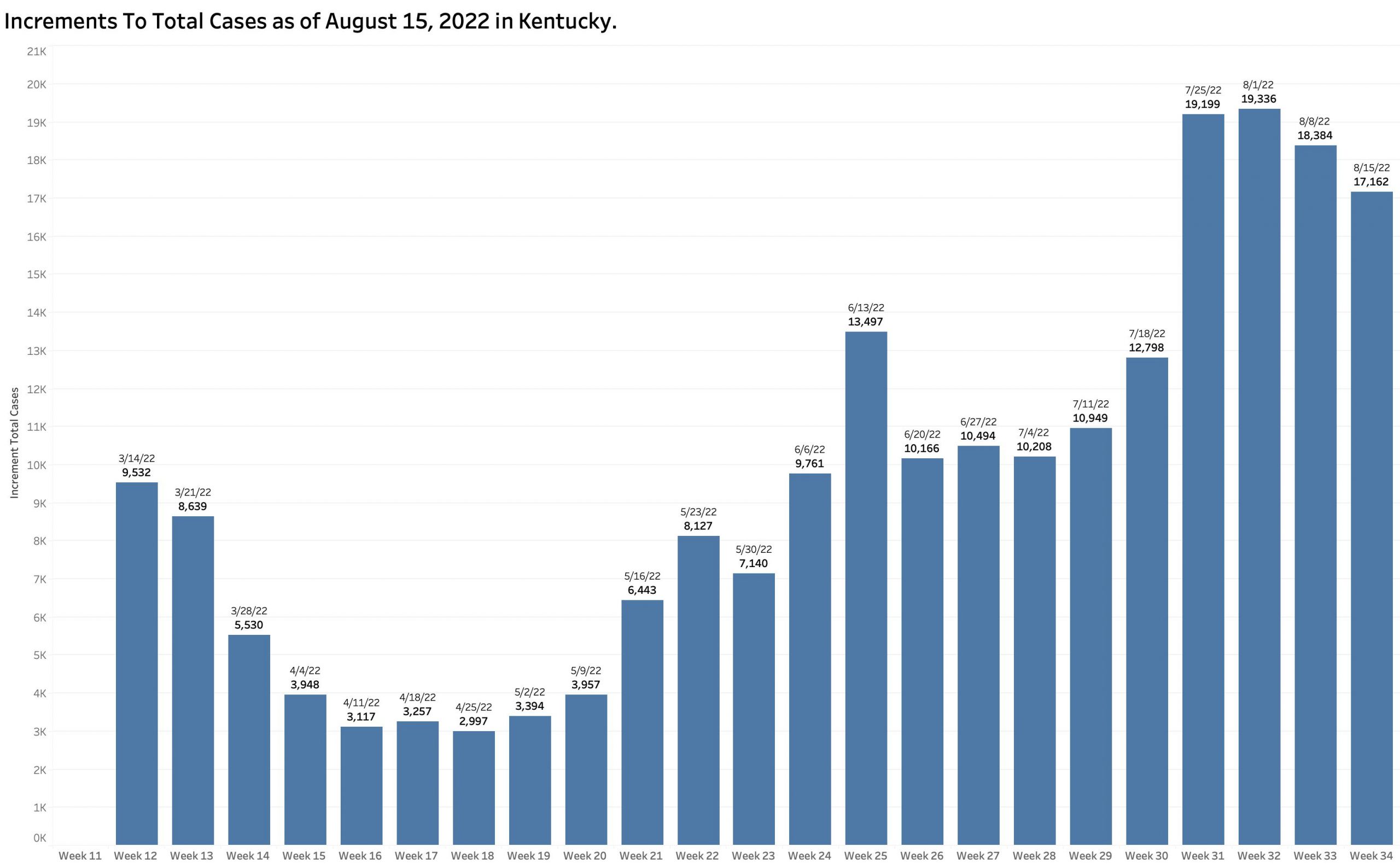
Incomplete reporting:
It can be assumed that for a variety of reasons that the number of New Cases as tallied does not reflect anywhere near the actual number of people who get infected. A second look at how Kentucky reports its cases reveals the ongoing weakness of our statewide identification and reporting systems that is shared widely across the nation. As part of its weekly summary of new cases, the state provides a running “Total of Cases.” In 7 of the 9 weeks of reports since June 20th, the increase in the aggregate counts of Total Cases exceeded the number of New Cases. The combined number of “New Cases” in past 4 weekly reports was 60,599 but the increase in aggregate Total Cases was 13,482 more than that – an amount of nearly a week’s worth of recent counts. These additional cases included those presumably identified and reported centrally to the State’s Public Health Department too late to be included in the counts of the individual current weeks. In my thinking, this means that we missed an opportunity to recognize the onset of an exponential rise in epidemic activity. Of course, if we lack the tools or willingness to do anything about it, this delay or incomplete capture of cases may not make much of a meaningful difference. Below is a chart of the weekly increment in Total Cases since mid-March. At least some of the peaks of the last 4 weeks would have shown up in a chart of daily New Cases.
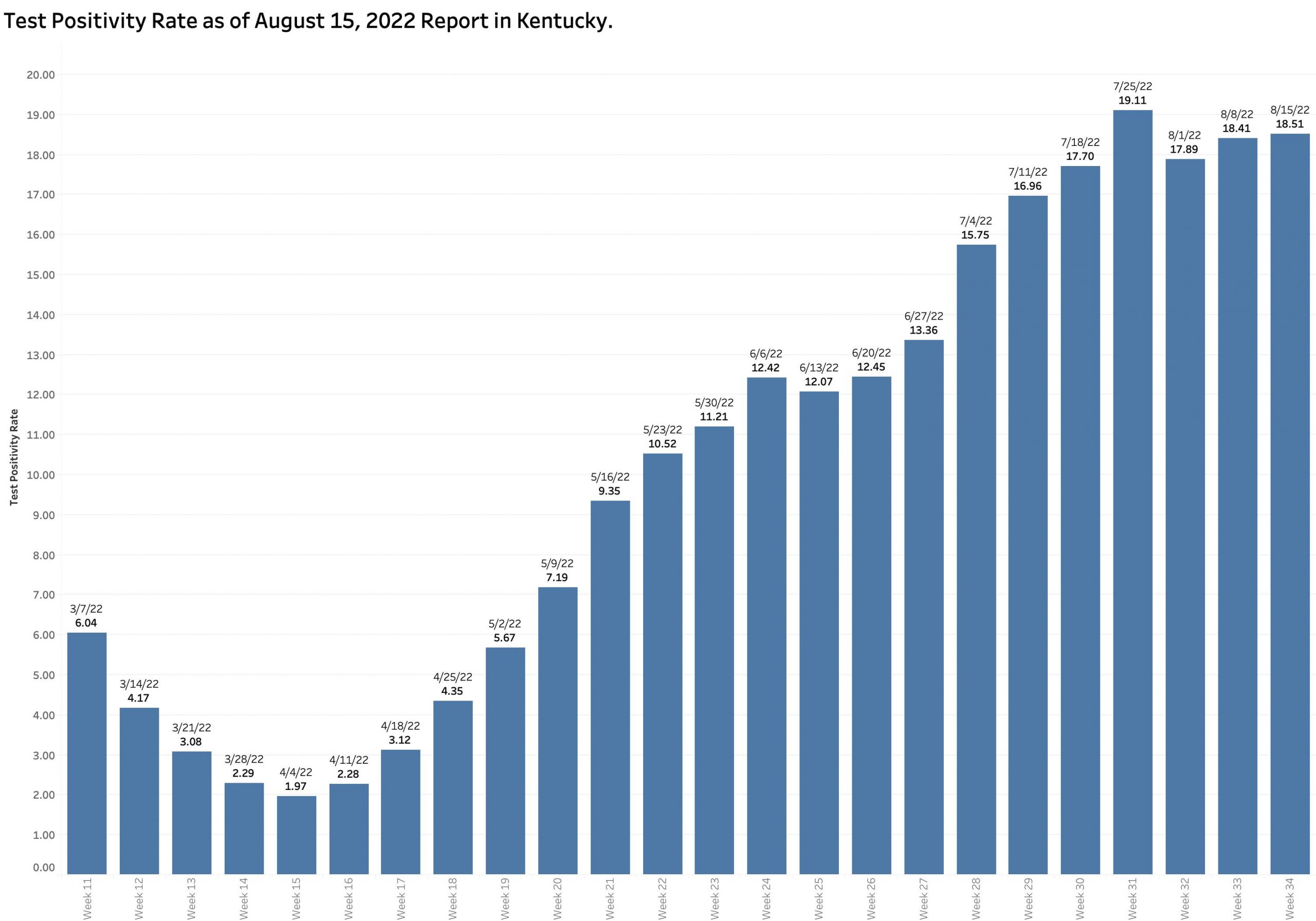
Test Positivity Rate:
Our Test Positivity rate remains high at 18.5% and in not going anywhere fast. In any case, this represents only a convenience sample of those getting tested for the virus by PCR RNA methods and reported electronically to the state. The number of individuals being tested weekly by PCR tests on which our TPR rate is calculated has not changed much over the past 4 months and may be declining.
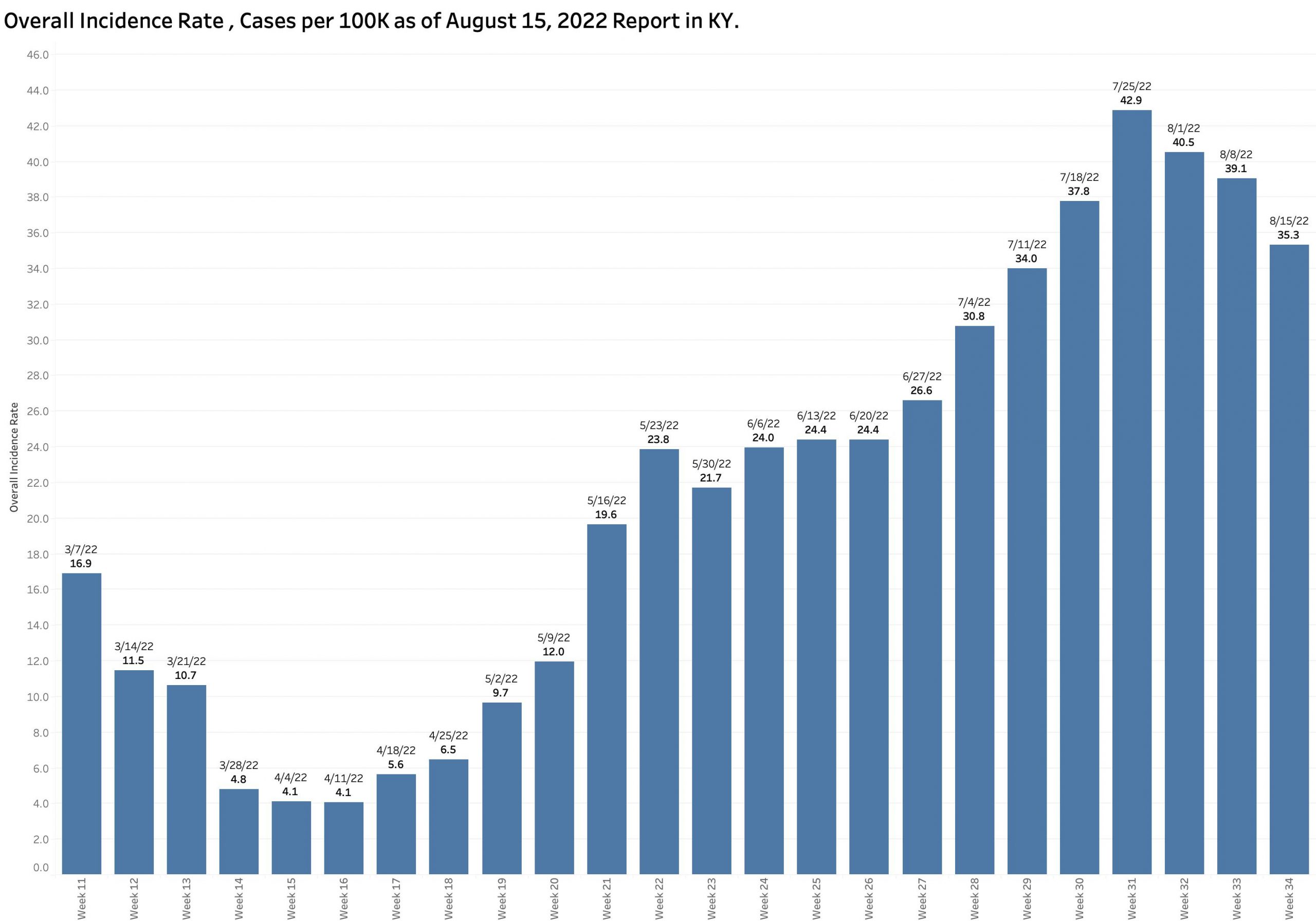
Overall Incidence Rate:
The number of New Cases per 100K population statewide as calculated is 35.3 per 100K and has been decreasing for the past 4 weeks from a high of 42.9 but remains quite high. A map of counties “in the red” on the state’s current Incidence Rate Map has been looking a little better in general, but 92 counties (77%) are still in the red with some counties consistently with very high rates leading the nation.
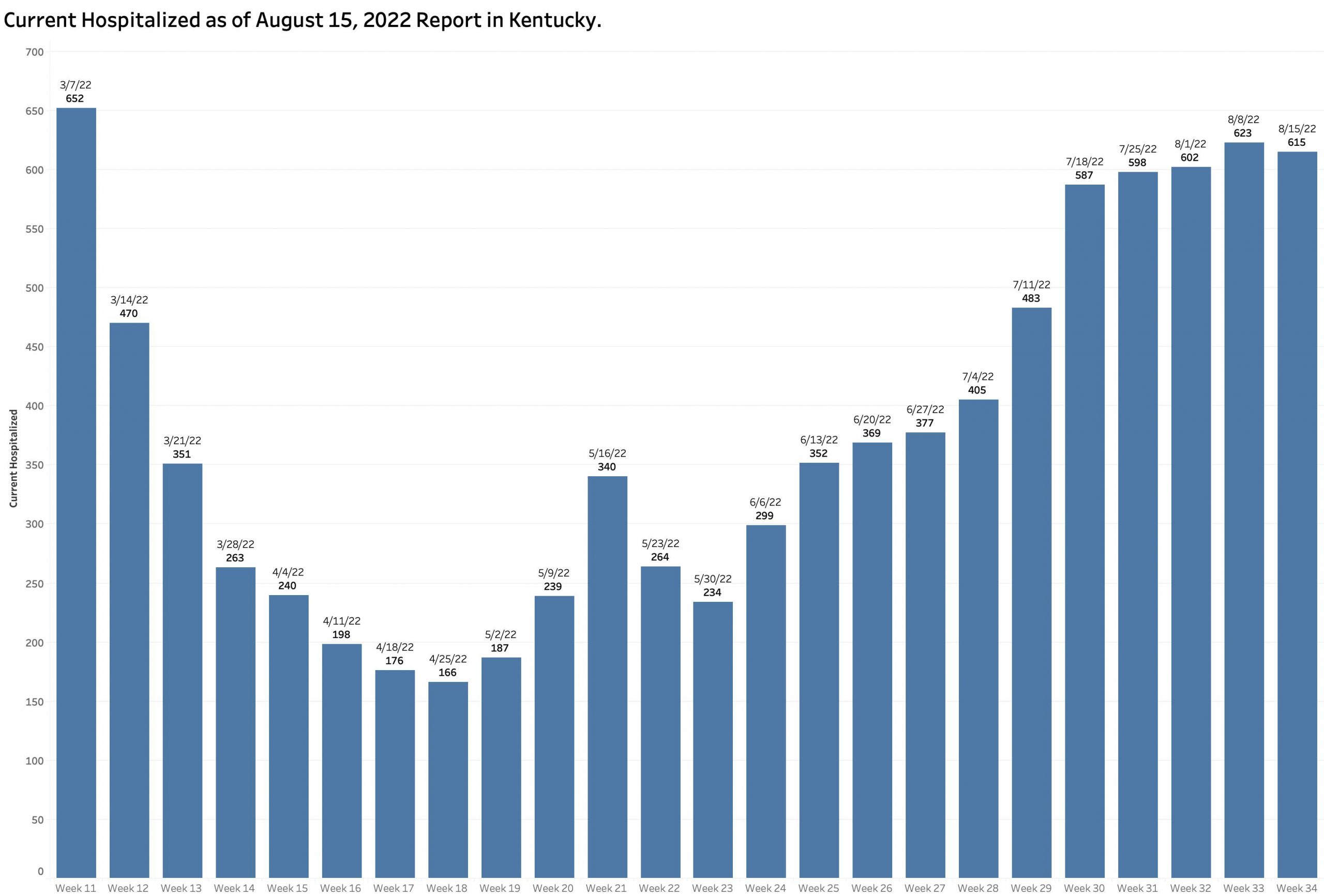
Hospitalizations:
Current hospitalizations remain high and are slowly increasing as counted. It cannot be said that infections from the current viral strain are clinically trivial. New strains will come which may be better or worse. More of my friends are getting infected or affected. How about yours?
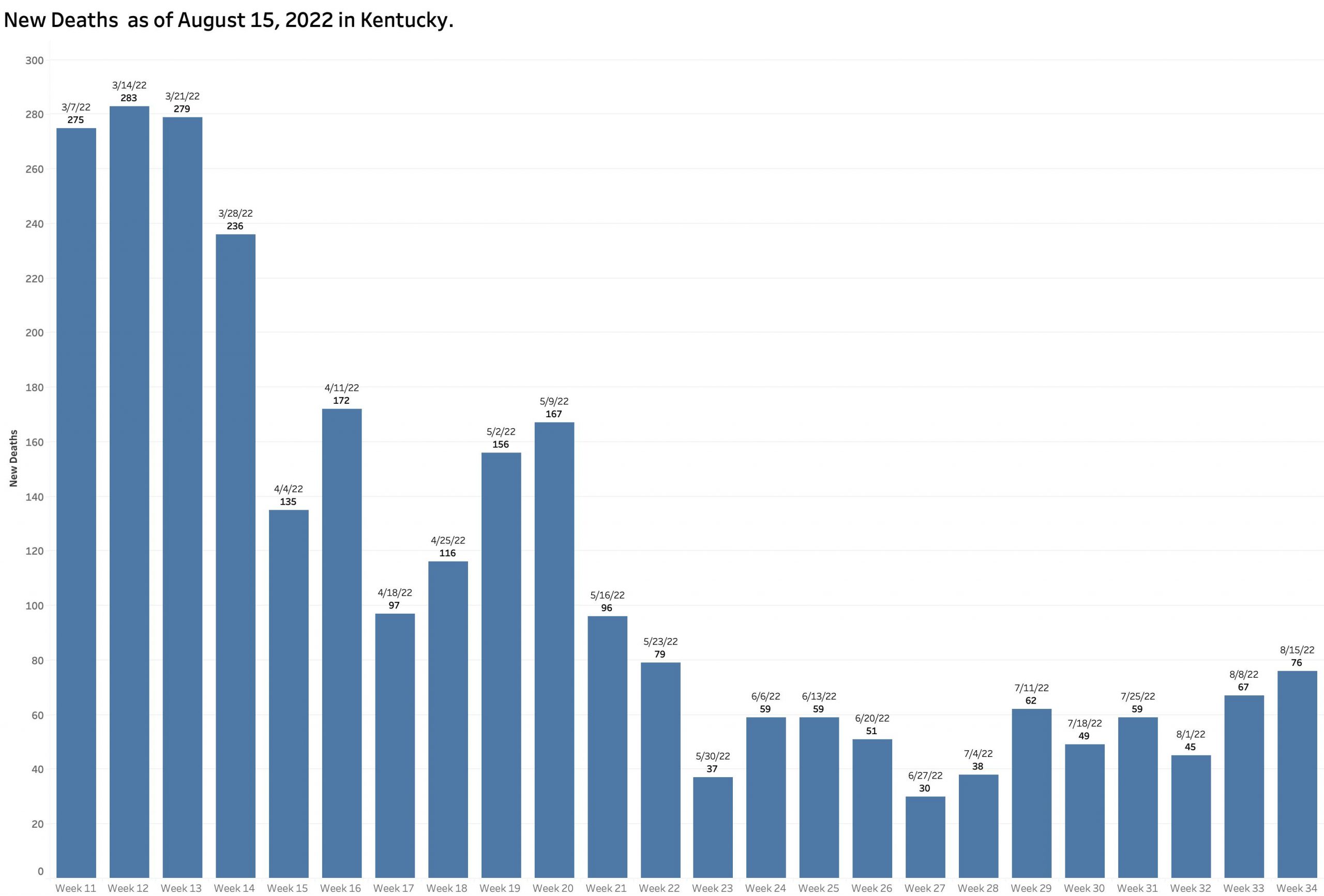
Deaths:
A background drumbeat of deaths continues.
In closing, I must confess that I am losing confidence in my ability or anyone else’s to judge where we are headed. I see the same shortcomings playing out in our current handling of the Monkeypox epidemic as were exhibited for the COVID one – or for that matter earlier epidemics from which we failed to learn or were unable to prepare for the next. The world is tuning inside-out in many geologic, environmental, and social respects. Such turmoil over the ages has been associated with disease and other disaster. We in our 21st Century United States are not immune from the old or new troubles.
Peter Hasselbacher, MD
Emeritus Professor of Medicine, UofL
Founder, Kentucky Health Policy Institute