Outlying prescribers of opioids and their drug-dependent patients are easy to find, but it is the standard of medical care in America that is fueling our current epidemic of opioid abuse, diversion, crime, and overdose deaths. These tragedies will not be solved by education, treatment, and law enforcement alone; nor by any amount of money we throw at the problem. The standard of care itself needs to be reassessed by the medical professions and the number and nature of first opioid exposures much reduced.
Long live the Prince.
He gave us the gift of his music. Might he give us anything else? Is there anything to be learned from his untimely death? As of this writing, there’s no longer any doubt that he died of opioid narcotic poisoning – more specifically of fentanyl overdose. It has also been reported that his addiction to opioids was long-standing, even as it was well hidden from his public. Current popular accounts attribute his opioid addiction to prescription drugs that were begun to treat unspecified injuries related to his vigorous stage performances– as if this somehow automatically legitimizes the use of opioids for musculoskeletal injury or chronic degenerative disease. A claim that “I can’t live without my opioids,” is in my experience generally a symptom of the opioid dependance itself, not the underlying disorder for which the drug was begun. That is why we use the term addiction. Of course there is a place in medical care for narcotic opioids, but we have strayed far from that place today.
Fentanyl is the new bad boy.
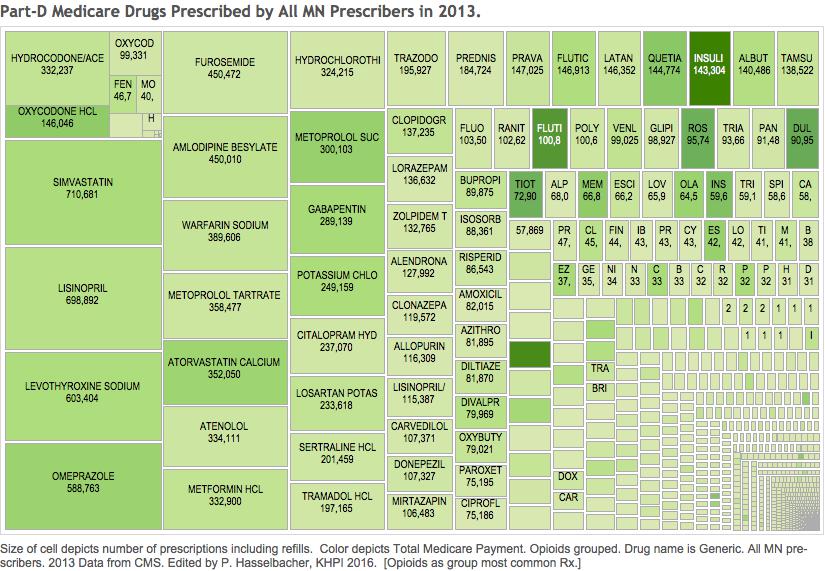
Many other current reported deaths attributed to opioid overdose involve fentanyl, either by itself, or added to preparations of heroin. There has been no evidence reported that Prince was a heroin-user, although the investigation into the circumstances of his death is not over. Fentanyl is, milligram per milligram, the most powerful opioid available on the market. It is well known that its potency takes some opioid users by surprise with not-infrequent fatal results. (A weekend full of deaths in a given community is commonly the result of a fentanyl-augmented batch of heroin.) It is not yet publicly known how long Prince might have been taking fentanyl. Did he come by his fentanyl illegally? Was it provided to him unlawfully by friends or supporters who obtained the drug in otherwise legal ways? Was the unscheduled landing of Prince’s airplane the day he died the result of a fentanyl surprise, or had he not yet been exposed to the drug. Did he acquire the medical disadvantage of being a “special” patient? I suspect we will find out. I also suspect that he acquired his fentanyl the same way innumerable other patients do – from their own local healthcare providers. Often, but certainly not always, the initial exposure to opioids is done with the best of intentions. In Minnesota, there are a few providers who have written colossal numbers of fentanyl prescriptions. From publicly available data, it does not appear that the physician whose name has most often been associated with Prince’s death is one of those. Continue reading “How Did Prince Get His Opioids?”