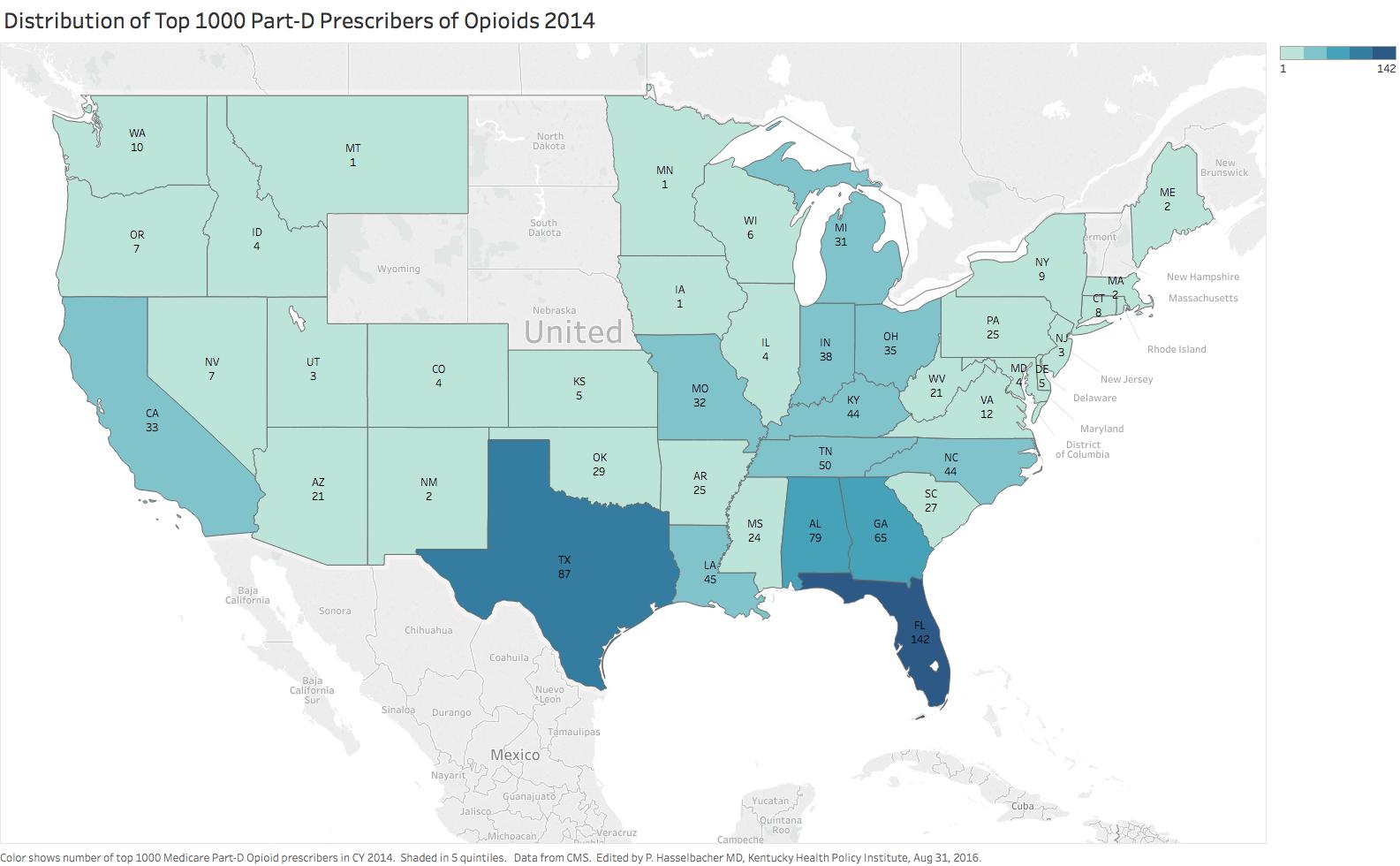
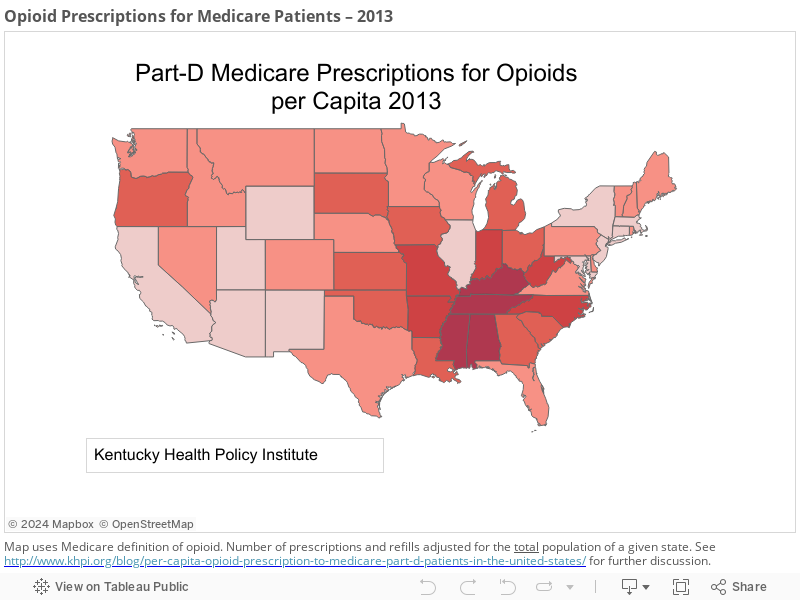
Kentucky’s high rates of opioid prescription must be reduced before even more prescribers are added. National data suggest that adding Physician Assistants to the prescribing mix is unlikely to reduce the number of opioid prescriptions written.
Louisville’s Courier-Journal this week featured an opinion piece by Andrew Rutherford, President of the Kentucky Academy of Physician Assistants, advocating for the passage of Kentucky Senate Bill 55 which would authorize physician assistants in Kentucky to prescribe controlled substances. Emphasizing the stakes involved in the proposal, articles later in the week reported on the latest rash of opioid overdoses in our region– presumably due to the inevitable fentanyl-enhanced “bad batch” of heroin. Several on-line commenters to the second articles suggested that since those who overdosed had made their own risky-decisions, that they should be permitted to suffer the consequences without an intervention of attempted resuscitation. It is suggested that this Darwinian mechanism would ease the opioid abuse problem. Unfortunately however, among the personal choices leading to opioid addiction is the choice to visit a licensed healthcare professional who, with good intentions or not, prescribes opioids. Once an individual becomes addicted, the concept of “choice” become irrelevant. A reasonable question to be asked is, “Do we really need to put more opioids in the hands of Kentuckians? My answer would be an emphatic no. Continue reading “Should Kentucky Physician Assistants Prescribe Controlled Substances?”