
 I learned today that the Republican-controlled Kentucky Senate passed a bill that would prohibit health facilities that currently run needle-exchange programs from giving out more needles than they receive from the substance-addicted people participating in the program. Only “one-for-one” exchanges would be allowed. The primary goal of any needle-exchange program is to prevent the spread of hepatitis, HIV, or other blood-borne infection that occurs when iv-injecting drug users share their equipment. Whether or not a program is successful is measured by changes in new infection rates. Kentucky could use a little help in that department. As of 2013, for at least the previous 4 years Kentucky led the nation in new reported cases of Hepatitis-C. That is not a place we want to be, including for reasons I will discuss below. The price we pay in gold and human misery is colossal, whether one abuses drugs or not! The 2013 data set from the CDC is the most recent available to me. I must assume that things only got worse since then.
I learned today that the Republican-controlled Kentucky Senate passed a bill that would prohibit health facilities that currently run needle-exchange programs from giving out more needles than they receive from the substance-addicted people participating in the program. Only “one-for-one” exchanges would be allowed. The primary goal of any needle-exchange program is to prevent the spread of hepatitis, HIV, or other blood-borne infection that occurs when iv-injecting drug users share their equipment. Whether or not a program is successful is measured by changes in new infection rates. Kentucky could use a little help in that department. As of 2013, for at least the previous 4 years Kentucky led the nation in new reported cases of Hepatitis-C. That is not a place we want to be, including for reasons I will discuss below. The price we pay in gold and human misery is colossal, whether one abuses drugs or not! The 2013 data set from the CDC is the most recent available to me. I must assume that things only got worse since then.
Prohibition and moralizing did not work for alcohol either.
It appears that many if not most of the Senate opponents of needle exchange programs in general are driven by puritanical or judgmental motives. There are certainly valid reasons to try to remove used needles and syringes from public spaces to avoid accidental injury, but that can and should be an independent initiative. The successful needle-exchange program in Louisville has made great progress in approaching a one-for-one exchange rate. The last thing we need in Kentucky is to have any of our towns or cities follow Austin, IN into the HIV and hepatitis blasted Hell out of which it will take several generations to climb.
Kentucky’s sons and daughters of families of all political parties are today sharing needles and other bodily fluids with HIV and hepatitis virus-infected individuals. One need not be a committed substance-injecting addict to be exposed. Healthcare workers are also at risk from needle-sticks. Our goal is to keep as many people healthy as we can through both prevention and treatment. Neither approach is easy, but that is not a reason not to try. Austin had the same warning we are being given now, but did little or nothing effective to stave off disaster. We need to do better. Moralizing will not do the trick. We must allow public health professionals to exercise their professional opinions based on best available evidence.
Perfect timing.
The notice of this attempt to tinker with Kentucky’s legal needle-exchange program was fortuitous. I was in the middle of preparing an article about the explosive increase in blood-born viral disease in Kentucky and the enormous cost to the Commonwealth of the promiscuous prescription of opioids, the cost of drug-assisted treatment for addicted persons, and the skyrocketing cost of the treatments for hepatitis. I am still working on the article, but here are a few of my findings.
Epidemics of hepatitis in Kentucky.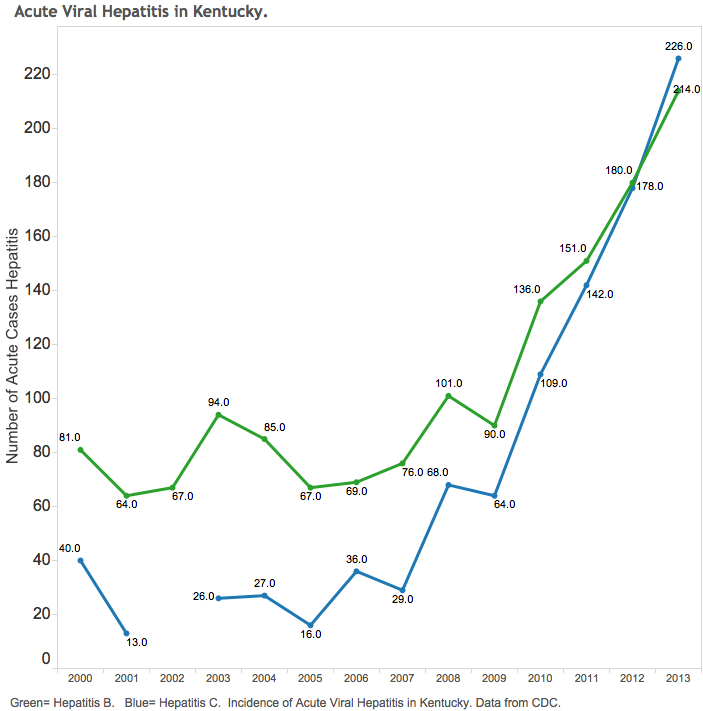
When scientists talk about an exponential rise in a chart, they are referring to a line that goes increasingly straight up with no end in sight – just like the one on the right depicting the number of reported cases of Hepatitis-C and Hepatitis-B in Kentucky over the last 14 years. The data comes from the Centers for Disease Control and Prevention. (I am still looking for more recent data. Can anyone help me?) The CDC estimates that because of under-reporting, the actual number of cases of Hepatitis-C is 20-times higher, and that of Hepatitis-B is 10.5-times higher. The rise in both viral causes of hepatitis began around 2010. I am preparing to add a line reflecting the incidence of HIV infection. I expect to see a similar exponential curve. (View an interactive graph here.)
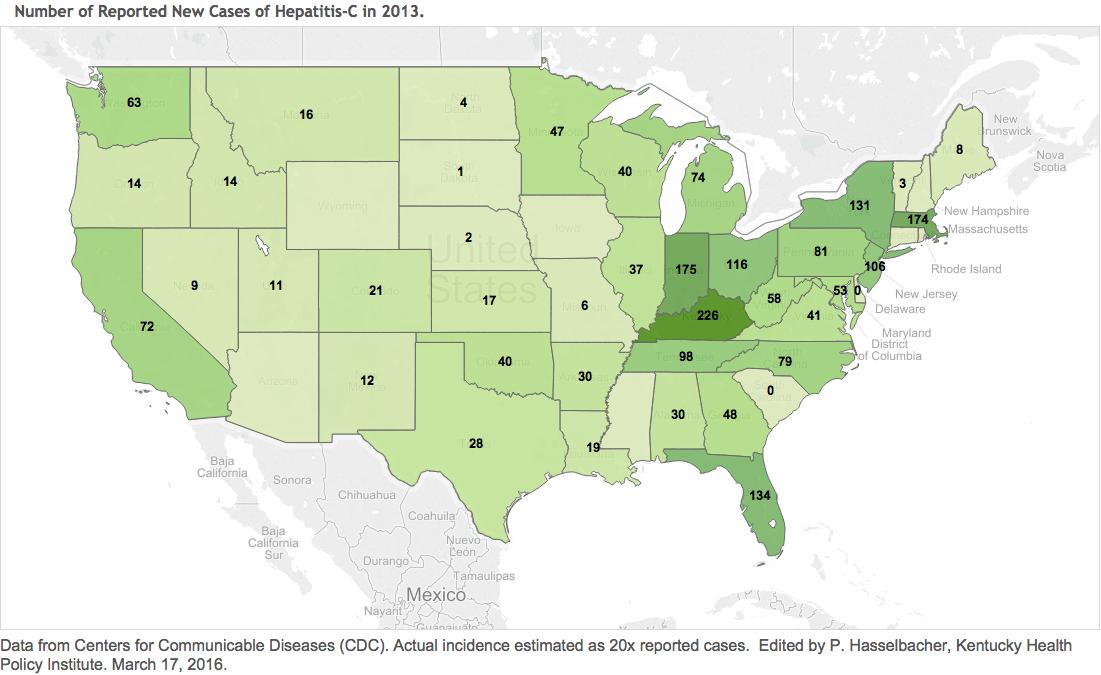
Kentucky wins the national hepatitis play-offs!
The thematic maps here show that Kentucky is leading all other state’s teams for the unenviable title of having the most reported cases of Hepatitis-C, and the highest rate of new infections per 100,000 men women, and yes, children. In fact, unless we are much better at reporting our cases than other states, we are running away with the game! (Click on the thumbnails on this page for full-size versions or look here for interactive versions of all the underlying data.)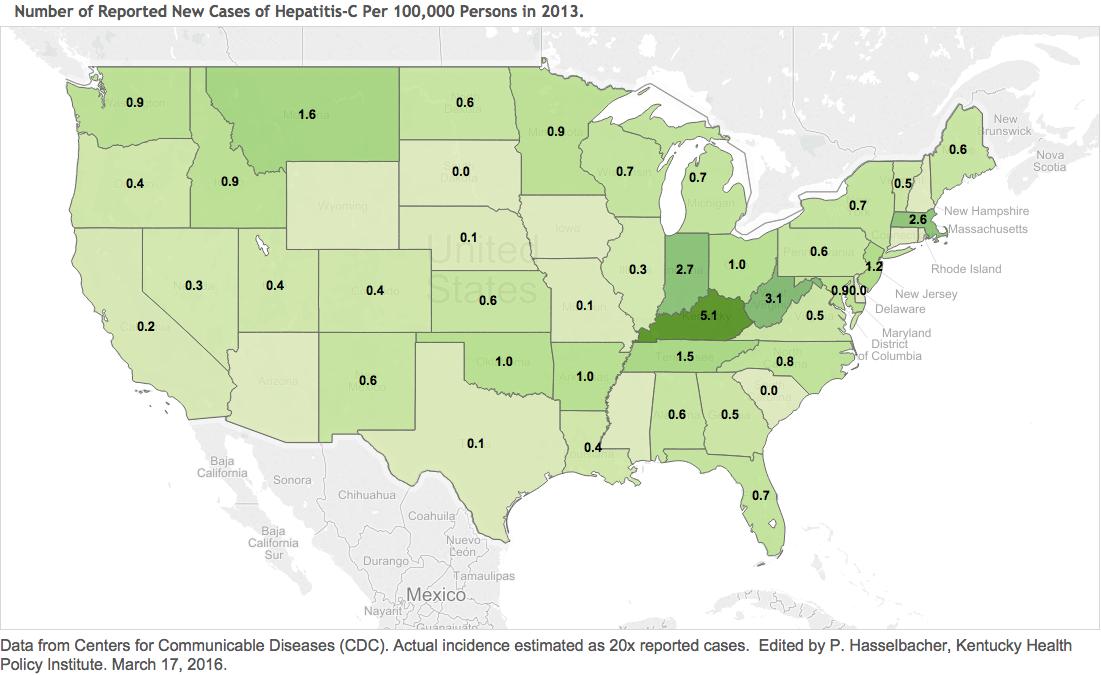
Stunning evidence of financial costs of promiscuous opioid use.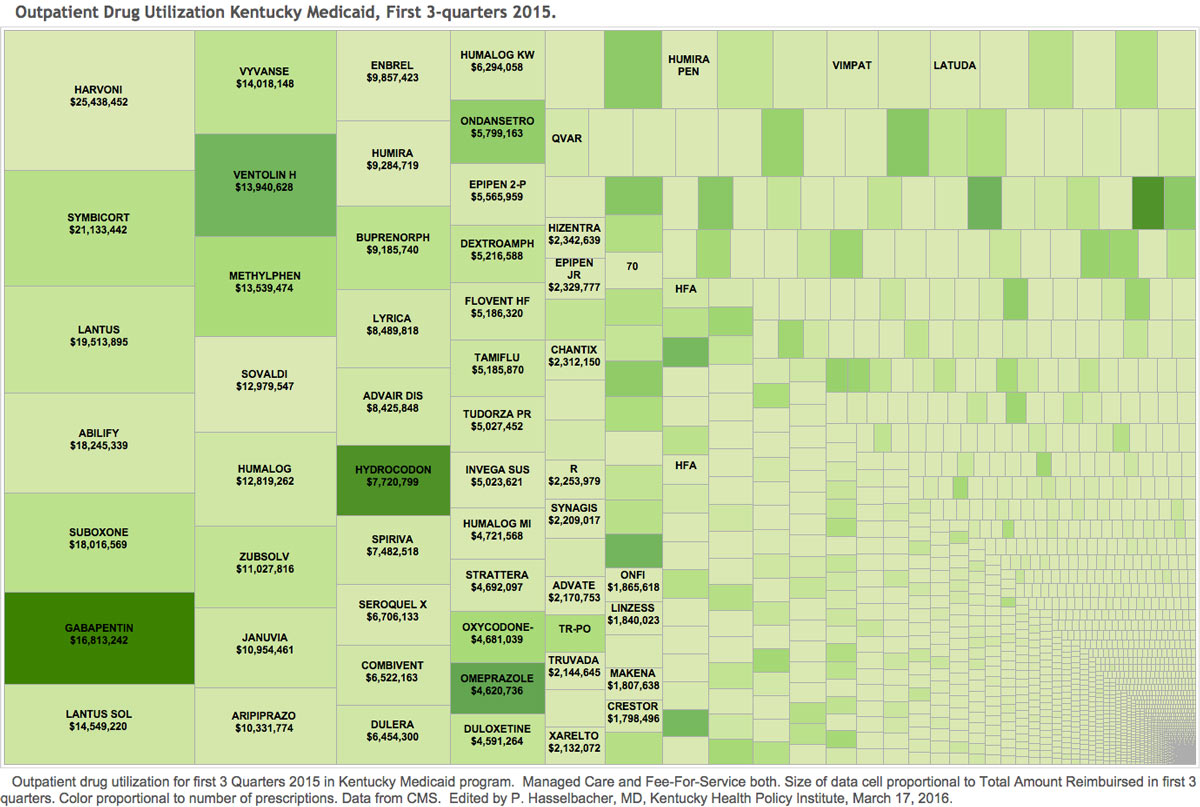
Just this week, CMS released its latest Medicaid Drug Utilization Database to the public – or at least the first three quarters of 2015. The Figure here depicts the amount of total reimbursement for each of 1801 individual brand or generic drug names prescribed to Medicare outpatient beneficiaries in both managed care and fee-for-service programs. Please refer to my earlier articles for background. The size of each data-cell is proportional to the total amount paid, and the color reflects the number of prescriptions written. (An interactive graph showing the underlying data for every cell is available here.) On the left side of the figure, only 38 drugs in the first four columns make up 45.5% of all outpatient and office drug expenditures! Of these, two drugs used for the treatment of Hepatitis-C alone cost $38.4 million comprising 4.6% of total Medicaid drug reimbursement! This is more than the top three prescribed opioids or fellow-travelling gabapentin at $29.2 million, or the two top drugs used for the treatment of opioid addiction (Suboxone and buprenorphine) at $27.2 million. These three categories of drugs among the top most expensive 38 cost us all $94.8 million, or 11.3% of total Kentucky Medicaid drug expenditures! Recall that further down the ranked list are many other drugs in the same categories which would add to the costs. These are big time numbers. To put things in perspective, among the top 38 most expensive drug names, 5 different human insulins cost $57.9 million (6.9%) with the oral drug Januvia making up another $11.0 million. (To convert these three-quarter year expenditures to a full year estimate, multiply by 1.33.)
Don’t do it.
Even if Governor Bevin and like-minded legislators are successful in rolling back Kentucky’s Medicaid program, the Commonwealth Commonhealth will still have to deal with the financial implications and the consequent medical complications upon our bodies politic. Sure we can toss our drug abuse problem back into the wilderness, but we will have to deal with it some day because it will drag us all down with it in both body and spirit. Remember too, that an across-the-board cut in Medicaid enrolment will condemn an army of diabetics to their own fates. Thus divided, we will fall.
Peter Hasselbacher, MD
President, KHPI
Emeritus Professor of Medicine, UofL
March 18, 2016
3 thoughts on “Legislative Tinkering With Needle-Exchange Program: Bad Idea.”
Comments are closed.